The push to reduce maternal mortality in the remote regions of Nepal
The government of Nepal's Safe Motherhood Program has introduced several initiatives to decrease maternal deaths by improving access to care in the country's remotest regions.
By Catherine Davison | Dec. 4, 2024




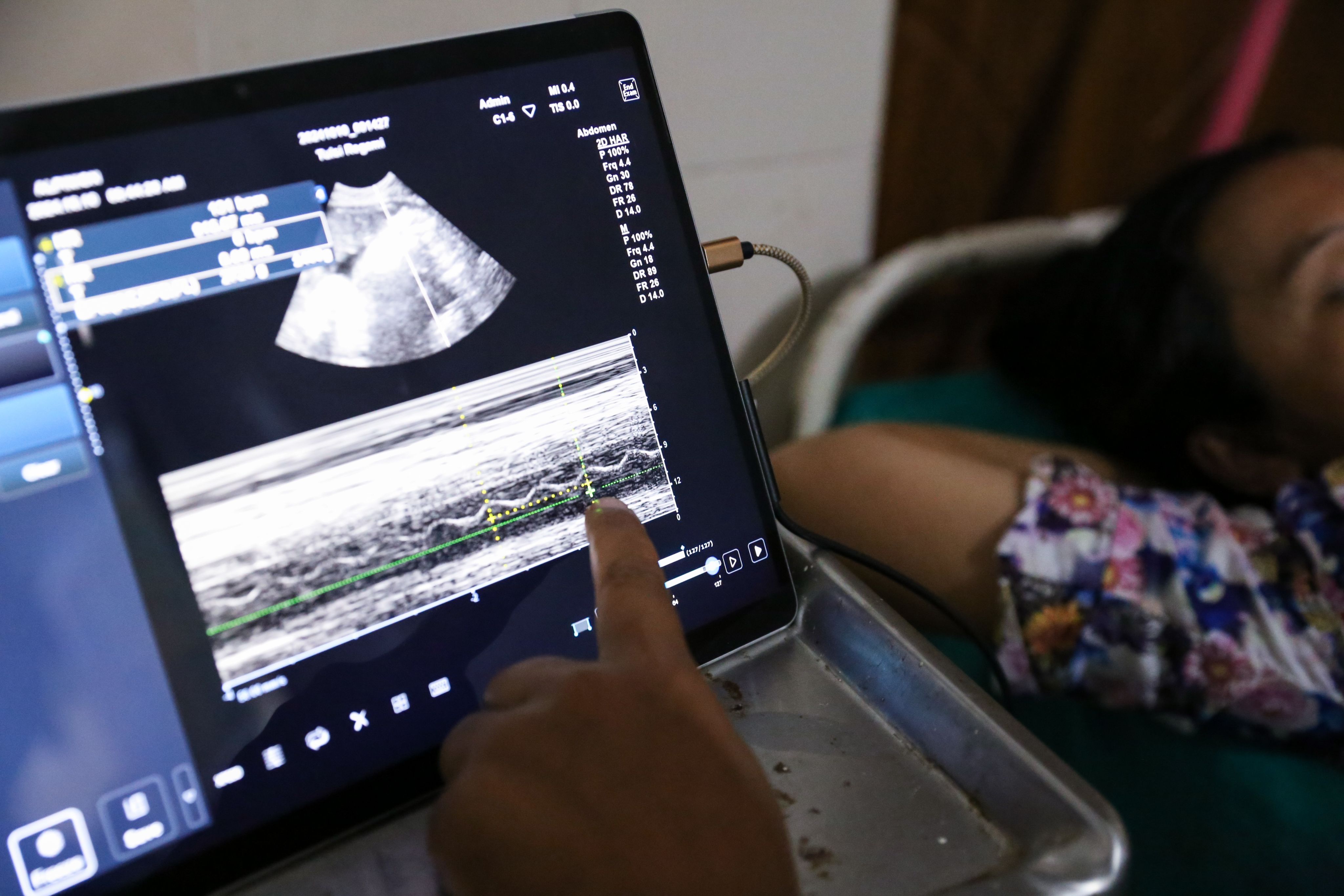
Karnali province, Nepal — Samjhana Salami pressed the sonogram lightly against a pregnant woman’s belly, and on the screen, the black-and-white image flickered: a heartbeat. However, the two women only had a second to marvel at the new life in front of them for the hospital was busy that day, and outside a queue of women waited to be seen.
It wasn’t always like that. When Salami started working as a nurse here 10 years ago, women coming for antenatal checkups were few and far between, she said. In the mountainous Karnali province of Nepal, most of the villages serviced by the rural municipality Naumule’s primary health care center are accessible only by foot; often, women have to walk for hours to attend antenatal checkups or deliver their babies. Most did not bother, choosing instead to give birth at home, leaving them at greater risk of complications.
But a push to decrease maternal deaths by improving access to care in Nepal’s remotest regions, where around 20% of the population live more than a 30-minute walk from the nearest health care facility, has changed that. In 2005, the government launched an incentive program that partially reimbursed women for the cost of transportation to health facilities, with women receiving up to 1,500 Nepali rupees depending on the region they live in. Four years later, the government eliminated fees for giving birth in a health care facility, with hospitals reimbursed expenses from the government’s health budget.







“That was a watershed moment for us,” said Dr. Bibek Kumar Lal, director of the health department’s family welfare division in Nepal’s Ministry of Health. When the program launched, just 10% of births took place in a health care facility, he said. Now that figure stands at almost 80%.
“Even four or five years back, there were lots of home deliveries happening in this part, but in the last year there were zero home deliveries,” Salami said.


Dr. Bibek Kumar Lal, director of the health department’s family welfare division in Nepal's Ministry of Health.
Dr. Bibek Kumar Lal, director of the health department’s family welfare division in Nepal's Ministry of Health.
Other initiatives were later added to what became known as the National Safe Motherhood Program, including the distribution of misoprostol in remote regions, a pill taken after birth to prevent postpartum hemorrhage, which is the leading cause of maternal deaths globally. Government payouts were introduced to incentivize women to attend at least four antenatal checkups — the World Health Organization recommends eight throughout a woman's pregnancy. And for those too far away to get to a hospital, once a month Salami and her colleagues carry a portable ultrasound machine, which plugs into a tablet, up into the mountains for remote antenatal clinics.


Source: National Population and Housing Census 2021: Nepal Maternal Mortality Study 2021. Kathmandu: Ministry of Health and Population; National Statistics Office.
Source: National Population and Housing Census 2021: Nepal Maternal Mortality Study 2021. Kathmandu: Ministry of Health and Population; National Statistics Office.
The efforts paid off. Nepal’s maternal mortality ratio, or MMR, dropped from 536 maternal deaths per 100,000 live births in 1996, to 151 in 2021 — a reduction of 72%.
Support from international partners has played an essential role in this success, providing funding, technical guidance, and training resources. Most prominently the United Kingdom, through what was formerly known as the Department for International Development, or DFID, contributed £71 million over a period of 10 years until 2010 — 9% of Nepal’s health expenditure.
However, in recent years donor interest has tailed off, highlighting a recurring issue in global health funding: The difficulty of translating short-term donor interest into sustained improvements in health care quality and access, especially for rural and marginalized populations. The share of external development partners in Nepal’s health budget dropped from 51.1% in 2006 to 20.6% in 2019, briefly shooting up again in 2020 due to the COVID-19 pandemic.
Despite initial improvements in the number of women delivering in health care facilities, the Safe Motherhood Program is now funded entirely by Nepal’s limited health budget, putting that progress at risk.
“It’s good that we have made some progress, but it’s not enough,” Lal said, adding that “any maternal death is a disaster.” Nepal has committed to reaching the United Nations Sustainable Development Goal target of reducing the MMR to 70 per 100,000 live births by 2030. But achieving this goal will require scaling up not just access to health care facilities but also improving the quality of maternal care, particularly in remote and underserved areas — something which will be a struggle given the constraints of Nepal’s already overstretched health budget, Lal said.
“I don’t see with the pace that we are now at, that we will reach that [goal],” he said. “We need to do a lot more, we need to invest a lot more, and that is quite a challenge in the current economic scenario.”
Quantity vs. quality


Part of the problem is that by focusing too heavily on the number of facility deliveries, Nepal became a “victim of our own success.” With numbers up, international funding dried up and donors turned their attention elsewhere “just like the seasonal fashion trend in Paris and Milan,” Lal said. With Nepal set to graduate from the list of least developed countries in 2026, those funding issues will be compounded, said Lal, who views that timeline “with a lot of apprehension.”
However, the push to increase facility deliveries was not accompanied by a corresponding improvement in service quality. An internal government review from 2019 found that while Nepal had “exceeded” targets on establishing new birthing centers, a “shortage of trained staff has severely hampered service delivery.” This meant that in reality, women would often go to a newly minted health care facility only to find that the necessary drugs or skilled service providers were not available — increasing the delay they faced in accessing care.
“Sometimes if you are providing service and it's not of quality, you do more harm than if you're not providing the service at all,” Lal said. While initially the number of institutional births was so low that resources were focused solely on increasing that figure, he said, once initial progress tailed off the government realized that they would need to pivot to improving the quality of care in order to sustain momentum.
To do this, the government works in collaboration with nonprofits such as One Heart Worldwide, an organization dedicated to preventing maternal and neonatal mortality, to ensure sufficient numbers of skilled staff, training, and equipment are available, particularly in underserved and remote areas of Nepal.
“We realized that was something we should have done earlier,” said Surya Bhatta, the executive director of One Heart Worldwide in Nepal. The nonprofit acts as an implementing partner, he said, supporting the government’s new focus on “improving the service quality and capacity building of the service providers working in these rural health facilities.”






In Naumule, Salami attended a training program to qualify as a skilled birth attendant, or SBA. For two months, she studied how to handle complications during birth and received training on using the portable ultrasound machine and doing basic antenatal checks to diagnose potential issues early on.
“There are still issues, but before they were not diagnosed,” Salami said. “Nowadays, they come to the health care center and we can detect the issues, and they get treatment on time.”
If problems are detected, patients are referred to a tertiary-level hospital in the nearest town to receive specialist care. A telehealth program also allows the SBAs to call doctors for advice in the case of an emergency. Since the initiative began in 2006, over 7,000 SBAs have been trained across Nepal.
In very remote areas, where referral to a hospital often means waiting for a helicopter — provided by the government for free in emergency cases where local care is not available — this training is especially important.
Two hours’ drive further up the mountain in the village of Paiti, Dilkumari Bista works as a nurse. As a new recruit, she hasn’t received her SBA training yet and said that sometimes her job can be “scary” when she is left to handle cases alone.
“It’s a risky job. If everything is normal then it’s fine, but if anything happens then who will be responsible?” she asked. She wants to get the SBA training so that “I can be more confident in my work when there are complications,” she said.


Specialized midwives


UNICEF and WHO recommend that all births be attended by an SBA, and the proportion of births attended by an SBA is an indicator of SDG 3 on good health and well-being. While trained SBAs have improved the quality of care in remote areas, what Nepal really needs are specialized midwives who have training on how to handle birth complications, Goma Niraula, president of the Midwifery Society of Nepal, said.
In 2016, Nepal introduced its first midwifery degree with support from the United Nations Population Fund, a three-year program that meets international midwifery standards and is designed to encourage the integration of midwives into public hospitals.
However, the expansion of the scheme has been slow, Niraula said; while Nepal will need 6,410 midwives by 2030, right now it only has 91. Currently, none of the graduates have been offered government jobs as midwives in public hospitals, and future sources of funding for their salaries remain unclear.
“The government lacks the commitment towards the deployment of midwives,” Niraula said.
Shanta Dangi, who graduated with a midwifery degree in 2022, works as a midwife at Paropakar Maternity and Women's Hospital in Kathmandu under a three-year program funded by UNFPA. Her sister, a nurse in Canada, is trying to persuade her to migrate, but Dangi said that she would prefer to stay in Nepal.
Shanti Dangi, a graduate from the new midwifery program, uses a cardiotopgraphy machine in Thapathali Paropakar maternity hospital in Kathmandu, Nepal, in October 2024.


“We want to help our country, we want to decrease our maternal mortality rate,” she said. “When the government recruits us for jobs over here, I will stay here, and I will provide the care to my own country.”
But without a government job on the horizon, she said she doesn’t know what she will do when the current UNFPA funding, which is supporting the hospital's midwifery program for three years.
The government’s national health care budget is stretched too thin to support the new graduates under government salaries, Lal said. “We are very good at adopting anything that comes [recommended] globally, without looking into the resource part,” he acknowledged, calling the situation “very unfortunate.” With graduates unable to secure jobs in Nepal, many are opting instead to work abroad — “which sadly, is not the purpose for which the investment is being made,” he said.
With “both an internal resource crunch as well as lack of support from the broader global donor community,” Lal said progress on reducing the MMR is stalling and warned that it may even see a reversal. “I am seriously concerned that we might lose the gains that we have made,” he said.
The last mile


In the remotest regions of Nepal’s mountains, however, even SBAs are often too far away.
Laxmi BK, who lives in the village of Paiti in Karnali province, had felt nervous about the birth of her first child. “I was scared because I didn’t know if I would live or die. Anything can happen,” she said. But reaching the nearest hospital meant walking for half an hour and then a three-hour drive along a bumpy dirt track. She ended up delivering her daughter Anuska, on the way, with no health care professional in sight.


Laxmi BK holds her 10-month-old baby, Anuska, in Paiti, Nepal, in October 2024.
Laxmi BK holds her 10-month-old baby, Anuska, in Paiti, Nepal, in October 2024.
Luckily, a backup option was at hand: a pill known as misoprostol, most commonly used to induce labor. When taken immediately after birth, it decreases blood flow to the uterus, reducing the risk of excessive bleeding. Postpartum hemorrhage is the leading cause of maternal death worldwide but some health experts are concerned that distributing misoprostol to expecting mothers will encourage home births.
Nepal first rolled out the distribution of the drug over a decade ago, as an alternative to oxytocin — an injection commonly given after birth to stop bleeding. Unlike oxytocin, however, misoprostol does not need to be refrigerated and can simply be taken orally, making it easy to self-administer in remote areas without access to health care centers. A pilot study in 2005 showed that it significantly reduced the incidence of postpartum hemorrhage.


Misoprostol available in the health care post is given to trained female community health volunteers in the surrounding area, who distribute the pills to women in the eighth month of pregnancy. Photo taken in Karnali province, Nepal, in October 2024.
Misoprostol available in the health care post is given to trained female community health volunteers in the surrounding area, who distribute the pills to women in the eighth month of pregnancy. Photo taken in Karnali province, Nepal, in October 2024.
In nearby Vitri Khola, Dilsara Thapa Magar also took misoprostol after going into labor in the middle of the night. With no cars available to drive her the two-hour distance to the nearest hospital, she gave birth in the kitchen. “I didn’t know where else to go,” she said.
“There is so much adversity around where you live,” Bhatta said. “If you live in very fragile and difficult geography, then not all of the women are going to make it to the health facility.”
The nonprofit facilitates misoprostol distribution in areas that are more than half an hour away from a health care facility. The pills are distributed by female community health volunteers, or FCHVs — women selected from each village to act as a point of care for pregnant women and new mothers.
After receiving training from One Heart Worldwide on the correct use of misoprostol, as well as other aspects of pregnancy care, FCHVs hand out the pills to women in the eighth month of pregnancy, instructing them to take it after birth if reaching a hospital proves impossible.

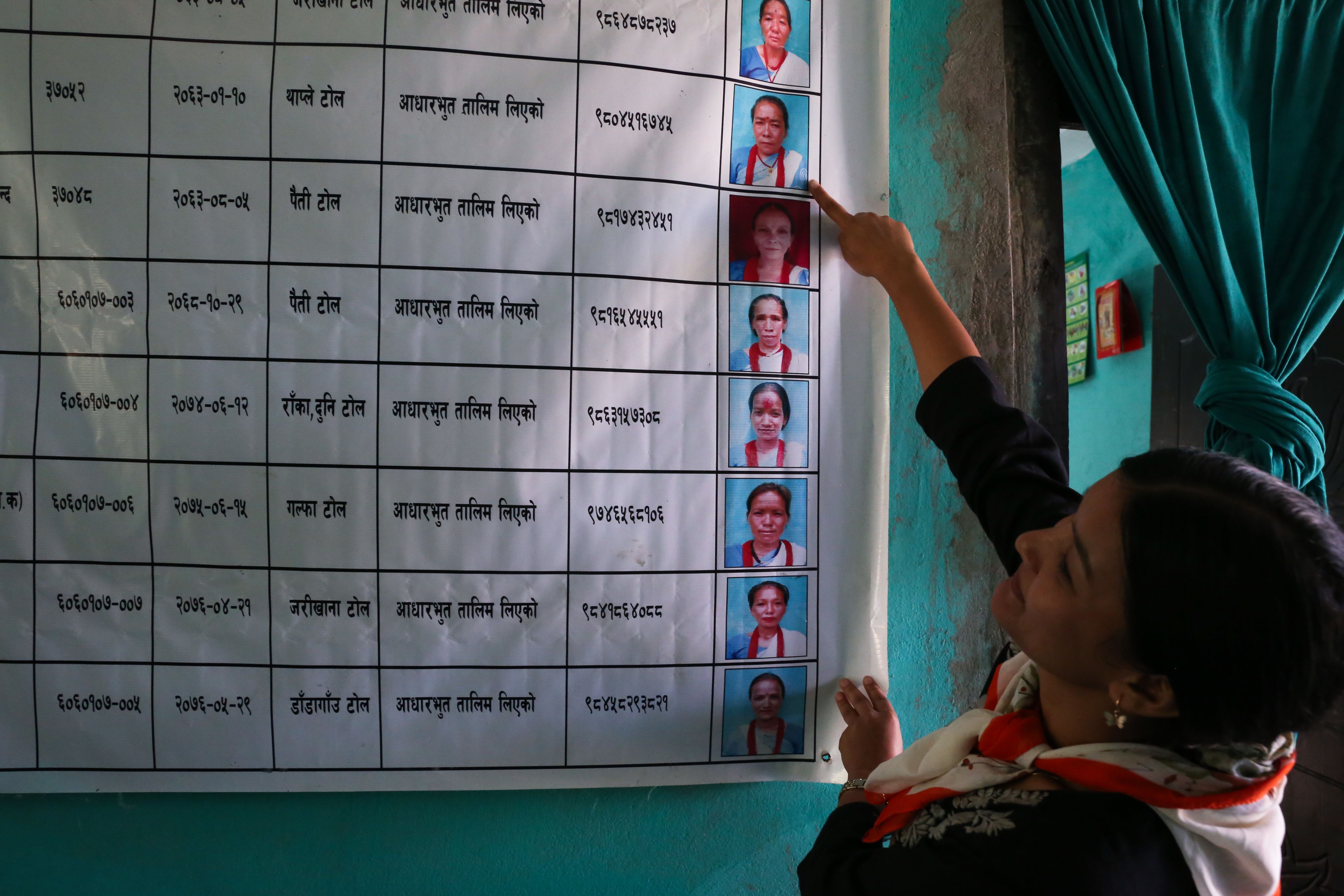




A list of local FCHVs at the health post at Paiti, Karnali province in Nepal, in October 2024.
Ratna Thapa, an FCHV in Naumule, walks for up to three hours to visit the homes of pregnant women and new mothers. She is proud of her work, helping to increase antenatal checks and hospital births.
“Before there were lots of maternal deaths, but now there are almost zero,” she said.
A neglected solution


The antenatal distribution of misoprostol is recommended by WHO “in settings where oxytocin is unavailable, its quality cannot be guaranteed, or skilled health personnel are not present to administer it,” according to official guidelines, which conclude that “it is likely to increase health equity and improve health outcomes.”
But despite this, the misoprostol program has not been rolled out consistently, with health care officials reporting regular supply shortages over the years.
In Paiti, Til Bahadur Kami holds the death certificate of his wife Karna. She had already given birth to six children at her home, located three hours away from a health care facility. But two years ago, she went into labor with her seventh child.
After the birth, she began “bleeding so much, much more than usual,” remembered her aunt Bhabisara. The family attempted to carry Karna down to the road, but she died on the way.

Til Bahadur Kami shows the ID card of his wife, Karna, who died in childbirth in 2022 from postpartum hemorrhage. Photo taken in Paiti, Karnali province, Nepal, in October 2024.
Til Bahadur Kami shows the ID card of his wife, Karna, who died in childbirth in 2022 from postpartum hemorrhage. Photo taken in Paiti, Karnali province, Nepal, in October 2024.

Bhabisara BK, the aunt of Karna who died in childbirth in 2022, in Paiti, Karnali province, in October 2024.
Bhabisara BK, the aunt of Karna who died in childbirth in 2022, in Paiti, Karnali province, in October 2024.
Sasikala Thapa, the FCHV who is in charge of the area where Karna lived, said that at the time there was no misoprostol available. She had received training on how to distribute the pill a decade earlier, but after a few years, the supply had dried up.
Karna’s husband Til Bahadur doesn’t know who to blame for her death. “I don’t know if it’s the government’s weakness or our weakness for being poor,” he said. “If we had that pill, maybe we could have saved her.”
This story is common across Nepal — and another example of where promising solutions have been hampered by insufficient training and uncertain sources of funding.
After the initial success of the pilot, some officials expressed concerns that distributing misoprostol would encourage home births. But Bhatta said that this belief is not supported by evidence and is a fundamental misunderstanding of the program, which should only be implemented in areas where home births are already highly likely.
At the local government level, there is “very little understanding of what that program means,” Bhatta said, and as a result “the program has not got the attention it should get.”
“Nepal is always bold in taking up innovations, but the problem is institutionalizing that and keeping up investment in that area,” he said.
One Heart Worldwide is now helping local government bodies to institutionalize misoprostol distribution in rural areas, by training local authorities and FCHVs on standardized methods of procurement, distribution, and usage. Its support, alongside the work of other international nonprofits, is proving essential for improving the quality of care and sustaining momentum, given the limited resources of the government and the reduction in support from country donors.
“I would love to be self-sufficient with our own resources,” said Lal, but “you need funds or resources for everything. You need human resources. You need training, you need commodities … I don’t think we will be able to reach there on our own.”


In Vitri Khola, Magar ended up having an uncomplicated delivery and said that she was glad that the misoprostol was available to her as a backup option. But she still believes that giving birth is dangerous, and contrary to those concerned that misoprostol will encourage home births, she is so determined to avoid giving birth in the kitchen again that she said she plans to use contraception until the road conditions improve.
“Next time, either I will give birth in hospital or there will be no baby,” she said.
Photos by Catherine Davison.
Produced by Patricia Esguerra.