Against the odds: Madagascar’s fragile polio victory
By Sara Jerving / Oct. 9, 2025
















Antranolahatra, MADAGASCAR — It had the vibes of a small town raffle night. Music blasted from a loudspeaker, and a woman stood at the front of the crowd with a microphone, calling out names, ushering them forward.


Children who were old enough danced — bobbed their knees, swayed side to side, and tapped their little toes. They cartwheeled, sang, braided each other’s hair, and dared each other to jump across a sand pit — giggling uncontrollably.
As the day wore on, some started causing mischief and were quickly scolded by adults with wagging fingers.
For these children, it was an epic party, but for the youngest, it was hardly so.

It was vaccination day for the remote village of Antranolahatra in southwest Madagascar, with a makeshift clinic hosted under the shade of two trees, surrounded by a cactus fence.
Mothers came forward with swaddled babies who wailed in their arms — thrashing to avoid the barrage of needles jabbed in multiple limbs. Older siblings were tasked with holding babies down, but for particularly squirmy ones, several adults joined in.
The mothers rocked and wiped away their babies’ tears — while also laughing at the dramatic displays.
This is all part of Madagascar’s effort to protect its children from vaccine-preventable diseases, including polio — a disease that paralyzes and kills.
It’s an incurable disease the international community has invested heavily in eliminating, although there are still flare-ups and spots of stubborn persistence.
Madagascar was declared free of wild polio in 2018, but between 2020 and 2023, it experienced an outbreak of type 1 variant polio with 56 confirmed paralysis cases, according to the Global Polio Eradication Initiative. The government and its partners responded with force — launching seven nationwide vaccination campaigns. There hasn’t been a case detected since September 2023, and the outbreak was officially declared over in May.
And though Madagascar has seen success, this work wasn’t easy. While the adage goes that it takes a village to raise a child — in the case of polio, it takes an international community to vaccinate one. Madagascar’s fight involved a symphony of people and organizations playing different roles — ranging from community health volunteers to international organizations.
It’s also involved myriad challenges: Vaccines must reach incredibly remote communities; there’s misinformation about them; resources are scarce; there’s dependency on unpaid health volunteers; cyclones disrupt campaigns; and there are complicated data collection systems.
And gains are fragile. There are still unvaccinated children, and the country struggles with significant sanitation issues. When poliovirus is present, it spreads through feces-contaminated environments. Open defecation is common across the country because toilets are considered taboo by some — as it’s seen as bad luck to store negative things such as human waste within a community.
The country is also amid violent protests over worsening water shortages and electricity outages — with calls for President Andry Rajoelina’s resignation. He recently dismissed his entire government.
And more broadly, foreign aid cuts — mainly by the administration of U.S. President Donald Trump — threaten the sustainability of global efforts to eradicate polio.
“It's not a one-time effort,” said Haingo Ranoharisoa, chair of the Rotary National PolioPlus Committee for Madagascar. “We still have a lot to do.”

Haingo Ranoharisoa, left, chair of the Rotary National PolioPlus Committee for Madagascar.
Haingo Ranoharisoa, left, chair of the Rotary National PolioPlus Committee for Madagascar.




A complex virus


The poliovirus is complicated. There’s wild polio — still endemic in Afghanistan and Pakistan.
But variant poliovirus is the most prevalent form globally. It happens when children vaccinated with oral vaccines shed a weakened strain of the virus in their feces, which can sometimes circulate among underimmunized and unimmunized people until it slowly mutates into a form causing paralysis.
This makes vaccinating entire communities critical so children aren’t exposed to threats from a contaminated environment.


There are three different strains of polio, and a combination of drops and injectable vaccines is used to counter them. Providing children in high-risk areas with both is considered the highest form of protection.
During Madagascar’s polio campaigns, children were given two doses of oral vaccines even if already vaccinated. Ultimately, Malagasy children are expected to receive four vaccine doses, including one injection.
The injection protects for all three types of polio — and is the only vaccine to do so. However, it doesn’t provide the same levels of intestinal immunity as oral drops. If a person is infected with wild poliovirus after receiving the injection, the virus can still multiply in their intestines and shed in their feces, to then possibly circulate in communities.

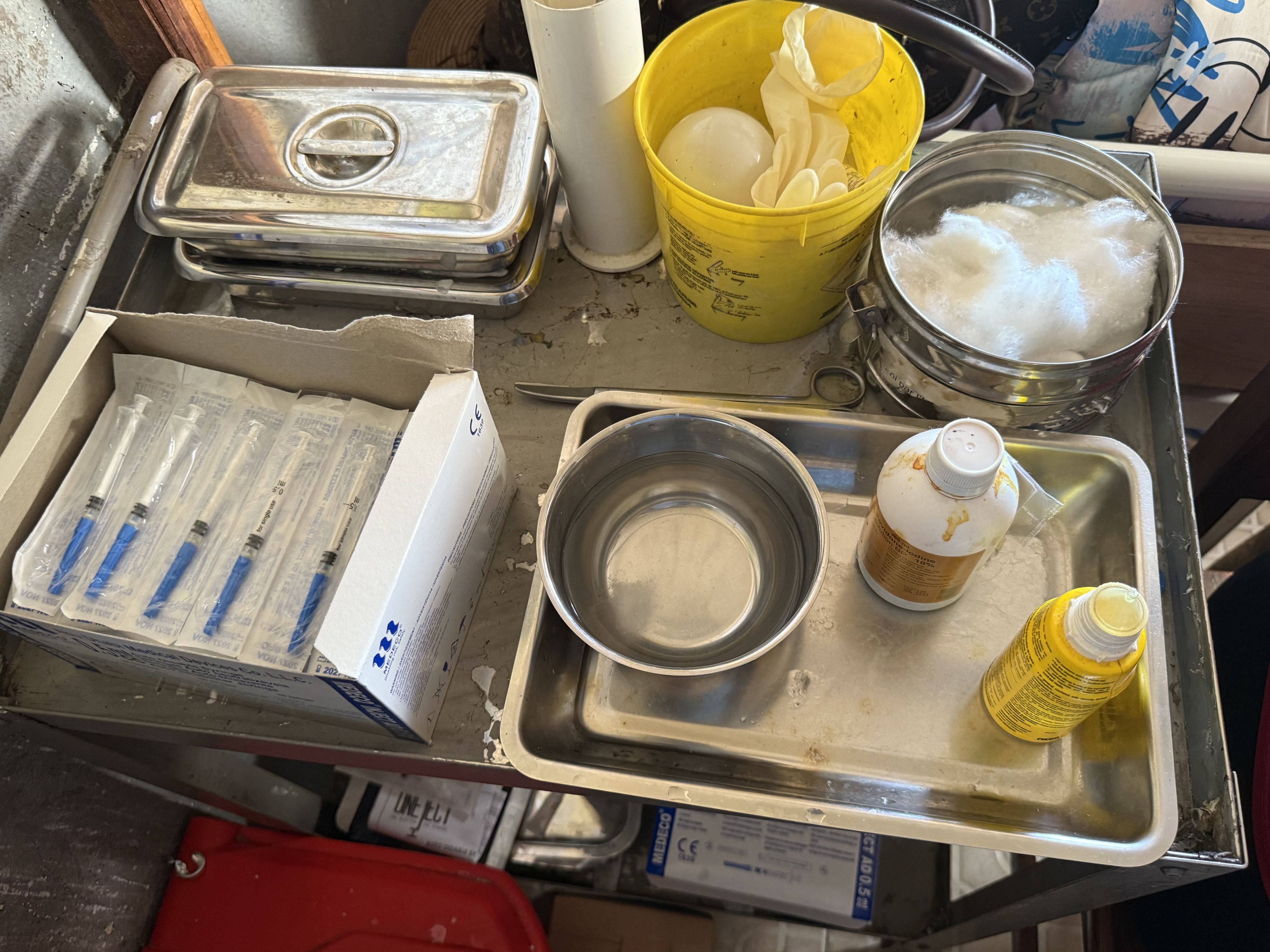
The oral drops are less expensive and easier to administer than injections, as they don’t require a health worker and sterile injection equipment, which is helpful in resource-stretched settings. The drops also have a strong ability to stop person-to-person spread, making them ideal for outbreak responses.
Type 1 variant poliovirus caused the outbreak in Madagascar.
“Variant polio type 1 outbreaks are a symptom of a low performing routine immunization system,” said Katy Clark, senior program manager at Gavi, the Vaccine Alliance. “There are many contexts around the world with poor sanitation, access issues, and hard-to-reach populations, but they don’t experience type 1 outbreaks. So, this was a unique situation that required special interventions — implemented at scale — to improve vaccination coverage.”
A fusillade of campaigns


To quell the outbreak, the Malagasy government and its partners launched four polio campaigns in 2023 and three last year — the last in October. About 63% of the population was vaccinated, including adults, as some were paralyzed during the outbreak.
The central government made the plan, and local levels executed it. It did this in partnership with the Global Polio Eradication Initiative, or GPEI, which includes six core partners: the World Health Organization, Rotary International, the U.S. Centers for Disease Control and Prevention, UNICEF, the Gates Foundation, and Gavi.








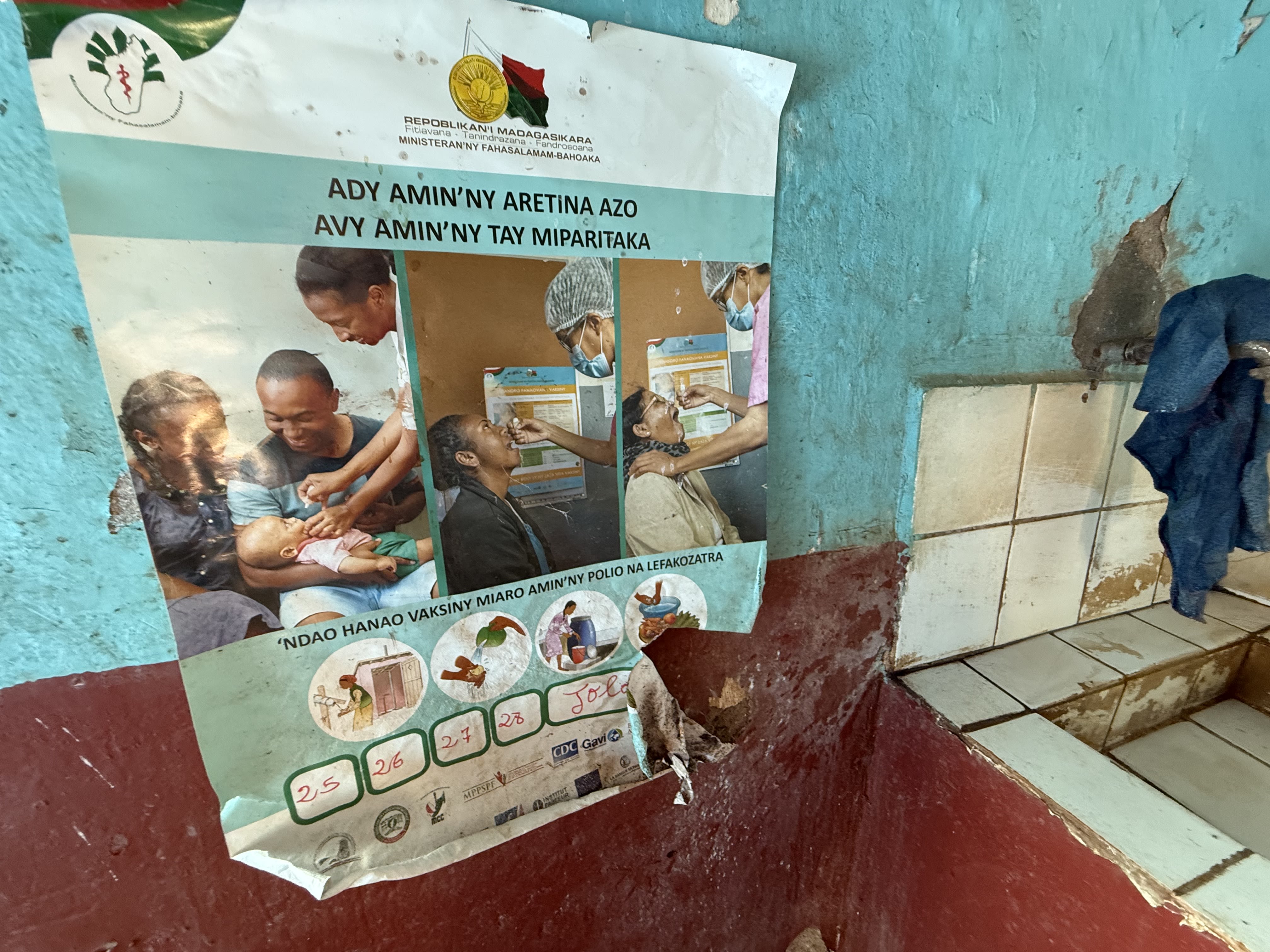
Local officials, such as chiefs and religious leaders, were tasked with getting communities on board, alongside community health volunteers. Posters were plastered around towns, and radio announcements blasted.
Mamiarisoa Vola Adrienne Josia and Ravaonindrina Antoinette were two community health volunteers on these campaigns.

They first went house to house, identifying children under 5 and convincing parents of the necessity.
During the campaign, they returned with a health worker and someone to register the vaccination.


Still drawn in white chalk on doors across the country are outlines of a little house that volunteers marked during the campaign.
Within the roof is the number assigned to the house, the upper floor has the number of inhabitants under 5 years old, and the bottom has the number of children at home and vaccinated when campaigners visited.
















During polio campaigns, teams are deployed nationwide for about five days.
The country was able to improve the effectiveness of campaigns, and successes have been credited to intensified surveillance, robust community engagement, and political will — for example, the nation’s president and first lady are strong vaccine advocates.

The government inaugurated a vaccine warehouse — the largest of its kind in Africa. President Rajoelina declared last year the “year of immunization,” and first lady Mialy Rajoelina became a vocal immunization champion.
“People listen to that type of messaging,” Gavi’s Clark said. “It wasn’t just a handshake meeting; they were really hardcore. … It wasn’t just words.”
UNICEF also appointed a young social media influencer to champion the fight against polio.
A Gates Foundation grant supports UNICEF in promoting government engagement on fighting polio and encouraging other vaccinations.
Now, the country is on alert: Posters plastered on health facility walls tell health workers to raise alarm and take stool samples if someone is paralyzed, and a new “state-of-the-art” laboratory to detect the virus, hosted at the Institut Pasteur de Madagascar, was recently transferred to the government.
From 2019 to 2023, more than a million Malagasy children under 5 years old were estimated to be without any vaccinations, but that’s been reduced by about 39.5%, according to the Ministry of Health.
Making it routine


While the campaigns were successful, they didn’t reach everyone.
When Michelin Rasoamihaja heard a knock on her door last October, she grabbed her daughter and grandchildren and hid behind the house until vaccinators left. She didn’t trust community health volunteers giving her grandchildren polio drops.
“We don’t trust the campaigns because the vaccinators are coming from our own community and they aren’t trained health professionals,” she said.

Michelin Rasoamihaj, right, with her daughter and grandson.
Michelin Rasoamihaj, right, with her daughter and grandson.




















But she’s fine with vaccinating her 1-month-old grandson at her neighborhood facility. She recently brought him to a routine vaccination day.

Some families also found the quantity of polio campaigns unsettling — growing suspicious of the necessity of having seven rounds.
Now, since there hasn’t been an identified polio case in over a year, the strategy has changed.
The country is largely dependent on routine vaccination — a combination of relying on children brought to health facilities and outreach to remote communities where it’s difficult for families to access clinics. The government also organizes, with partners, nationwide campaigns offering an array of vaccines.
“If we stop this routine vaccination, we will have an outbreak again,” Rotary’s Ranoharisoa said. “It will never end: We will have to do it nonstop.”
Vaccination day under the trees in Antranolahatra village was an example of that type of outreach.
A married couple who work as community health volunteers laid the groundwork.
The wife, Marie Laurence Tsirakofa, has been a community health volunteer for 22 years. Her husband, Koto Jean, left his role as village chief in 2010 to join her.
In the lead-up to vaccination day, they traveled around their community identifying kids needing vaccines and handing out referral slips.
At the beginning of vaccination day, they gathered over 70 children’s vaccine booklets and called them in turn. Jean sat with his glasses at the tip of his nose, furiously cross-checking vaccination books against their own records.
Doctors for Madagascar, an international nongovernmental organization, supported this vaccination day as part of work funded by Gavi, Bayer Foundation, and UBS Optimus Foundation.
Many kids received their first polio vaccine that day. This included 7-month-old Dauphine, whose mother had been farming in a distant field during the last polio campaign and missed the initial opportunity.
The long trek










The winding roads of Ifanadiana district in the eastern region of Madagascar — about a day's drive from Antranolahatra village — cut through rolling mountains dappled with eucalyptus trees and terraced rice fields.
Mothers tend to walk with babies in one arm and baskets on their heads. Vendors will sell black strips of vanilla and deep-fried bananas. Small herds of zebu — or humped, horned cattle — are shepherded amid bustling markets.
The air is usually filled with wafts of flowers and echoes of babbling brooks.
The landscape is equally breathtaking, as it is a logistical nightmare.
Vaccines are distributed to districts, but must then be delivered to health facilities. Some are nestled far away from main roads that require crossing a river and mountainous terrain to reach.
And so vaccines aren’t always in stock — people could travel long distances only to return home with unvaccinated babies.
A UNICEF and WHO assessment found that long distances to health facilities were the leading barrier to vaccination in Madagascar, followed by families not having the time and being unaware of its importance.
“It takes a long time to get vaccines where they need to go — to that last mile. If you don't have vaccines, you don't have routine immunization happening,” said Andrea Thompson, who leads the Gates Foundation’s polio work in Madagascar.










Pivot, a Malagasy NGO, is one of the organizations assisting the government in getting vaccines to remote facilities in a few districts.
It can take three days to reach the furthest health facility in the Ifanadiana district — just one way — with the round trip taking about six days.
Reaching the most distant facilities is a major challenge.
As two of Pivot's motorcycle drivers, Rakotonirina Malala Dieu Donné and Randrianarison Blaise Mahmias, explained, they can only get so far on their bikes before the terrain becomes too rough to continue.
And so they meet someone from the health facility who may have walked a day to meet them. That person must then travel another day, with a cold box slung over their shoulder, to bring the vaccines to the health facility.
Because of the tricky landscape, Pivot’s drivers deliver vaccines in pairs.
Mahmias held up a picture on his phone of two sticks used as a rickety bridge. One driver guides the motorcycle over the bridge on foot from the front, and another from behind.
But it’s also a job the two drivers love — they’ve been enamored with motorcycles since their youth — they make a game of racing one another on the open roads.
“It’s an adventure,” Mahmias said.







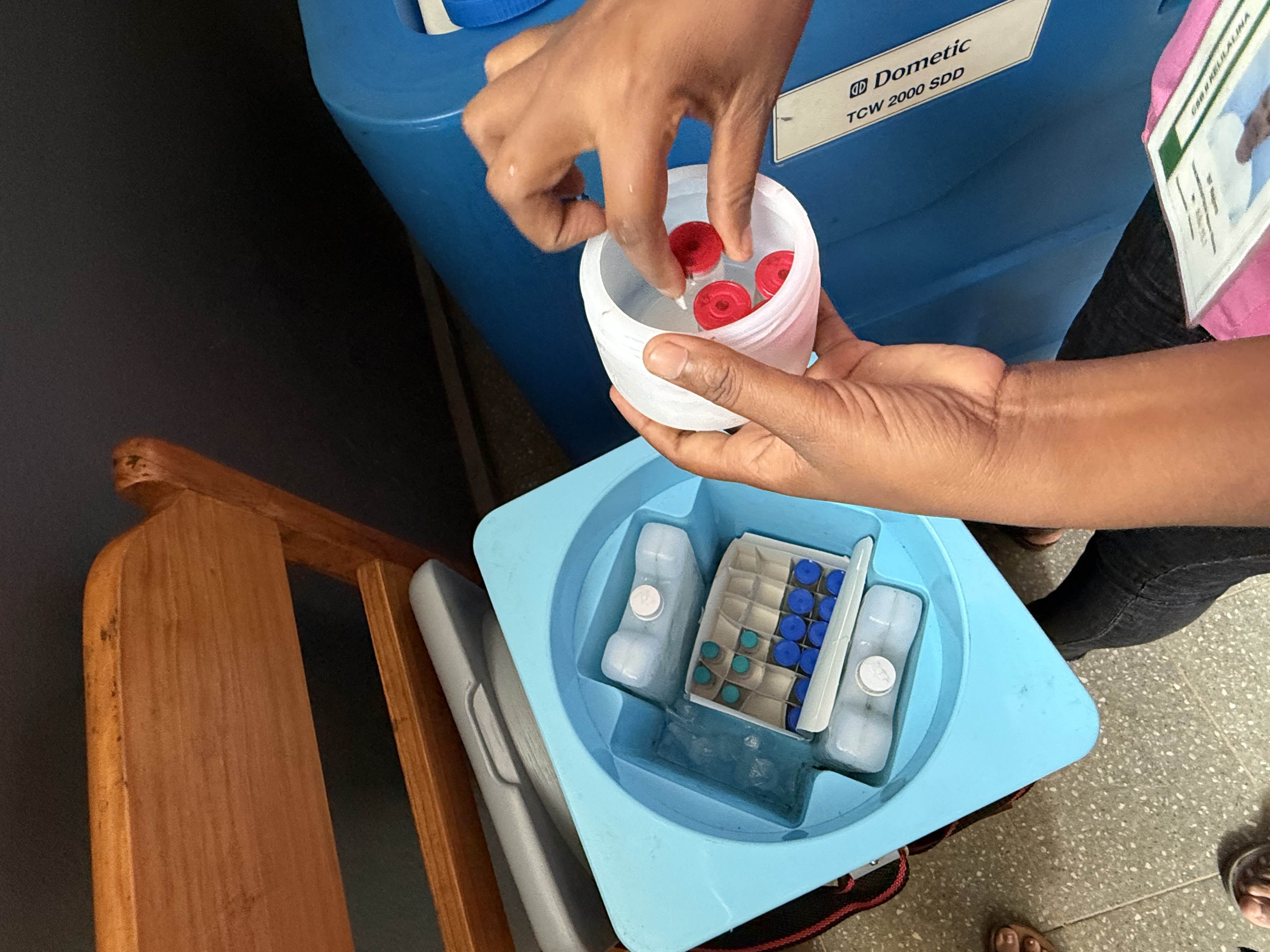






Once at the health facility, vaccines need refrigeration.
About 75% of basic health facilities in Madagascar lack electricity or only have a solar refrigerator. Some refrigerators are out of service, with maintenance challenges.
This means health facilities can’t stock up.
And cyclones complicate this further. With floods, even motorcycles can’t pass roads — and sometimes the drivers must negotiate with farmers to dig tunnels to divert water.
According to Pivot’s research, in 2023, 35% of children aged 12 to 23 months in the Vatovavy region, where they work, received no vaccinations. Nationally, in 2021, 18% of children the same age hadn’t received any vaccinations.

On a recent morning, Dr. Andriamanalina Manatenasoa Miora, the chief of Kelilalina Health Center in Ifanadiana district, talks to mothers outside her clinic about vaccination benefits. Pivot used to pay her salary, but now she’s integrated into the government’s system.
At her clinic that morning, a baby wails when a polio injection enters his little thigh. The mother leans over and dribbles breast milk on it for soothing. She walked three hours for her son’s final polio dose.
Falling from the sky






















Hundreds of miles away at the two-room Bemanga health facility in southwestern Madagascar, there’s no internet, electricity, or bathroom, and there's limited cellphone service.
It’s about three hours from the nearest city, and to reach it, you must go off-road for about an hour on a bumpy path with ravines and terrain that shapeshifts from sand to soil.
The clinic serves over 4,200 people.
Zapolino Sylvana Razanantsoa, a nurse, was sitting on the observation room bed one day when a message popped up on her phone.
She realized that was one of the few places her phone had service. She nailed a plastic brace on a wooden window and now must stand on the bed, leaning her head against the window to receive calls.
That’s how she receives vaccines. She knows she will receive a call on certain days saying vaccines will fall from the sky, landing in a nearby field in about half an hour.
It’s a drone project, which started last October in three regions, funded by Gavi and implemented by PSI Madagascar, in partnership with the government.
And while it’s not perfect — sometimes vaccines break upon landing — it’s more reliable than when they previously waited for land deliveries.

Dr. Razanakolona Herimaminiaina Robert, medical inspector for Sakaraha district.
Dr. Razanakolona Herimaminiaina Robert, medical inspector for Sakaraha district.
Dr. Razanakolona Herimaminiaina Robert, the medical inspector for Sakaraha district, said that the majority of his district's health facilities use drones for vaccine delivery, particularly those located over 30 miles from Sakaraha town.
He said reaching children “perdu d’vue,” or “lost from view” in French, is one of the health ministry’s greatest challenges.
For his district, there’s a particular problem with nomadic communities artisanally mining sapphires. When the gem reserves are depleted, they pick up their lives, moving to other gemstone deposits.
The district currently uses mobile clinics to reach isolated and nomadic populations, but it needs more of them to meet the demand. But they are expensive, Dr. Robert said, with costs such as fuel.
Ravelomahafaly Herimaminiaina Christian, a technical adviser at Doctors for Madagascar, said he knows of a community living over 85 miles from a health facility.
‘Heart and soul’


In a country with limited resources and health facilities in hard-to-reach areas, the work of community health volunteers is critical in keeping health systems afloat.
They “are the heart and soul of the communities,” Gavi’s Clark said.
“Without their intel, without their knowledge of why people act the way they do, we would not be successful,” she said. “They're the ones who know the communities, they know the houses, they know the reason for hesitancy, they're the ones, when they knock at the door, they’ll get a response.”








“They are convinced that a free thing can’t be good for them,” said Faneva Toaviniaina, a community health volunteer in Sakaraha.
“Especially if it’s from foreigners; they can’t do good things like this for free.”
There’ve been a few times where parents say to her, “If my child dies tonight, I’m going to come for you.” In response, she dropped the polio vaccine into her own mouth to prove safety.
Another community health volunteer, Yvonne Crystelle, said about one-third of the children she assessed through her work with Doctors for Madagascar hadn’t yet been vaccinated for polio.
Organizations such as UNICEF, Rotary International, Scouts, and the International Federation of Red Cross and Red Crescent Societies have worked with the government in dispelling polio vaccine misinformation, in partnership with community health volunteers.
Two of the polio campaigns targeted adults — and that was particularly challenging since vaccinating adults isn’t common, Rotary’s Ranoharisoa said.
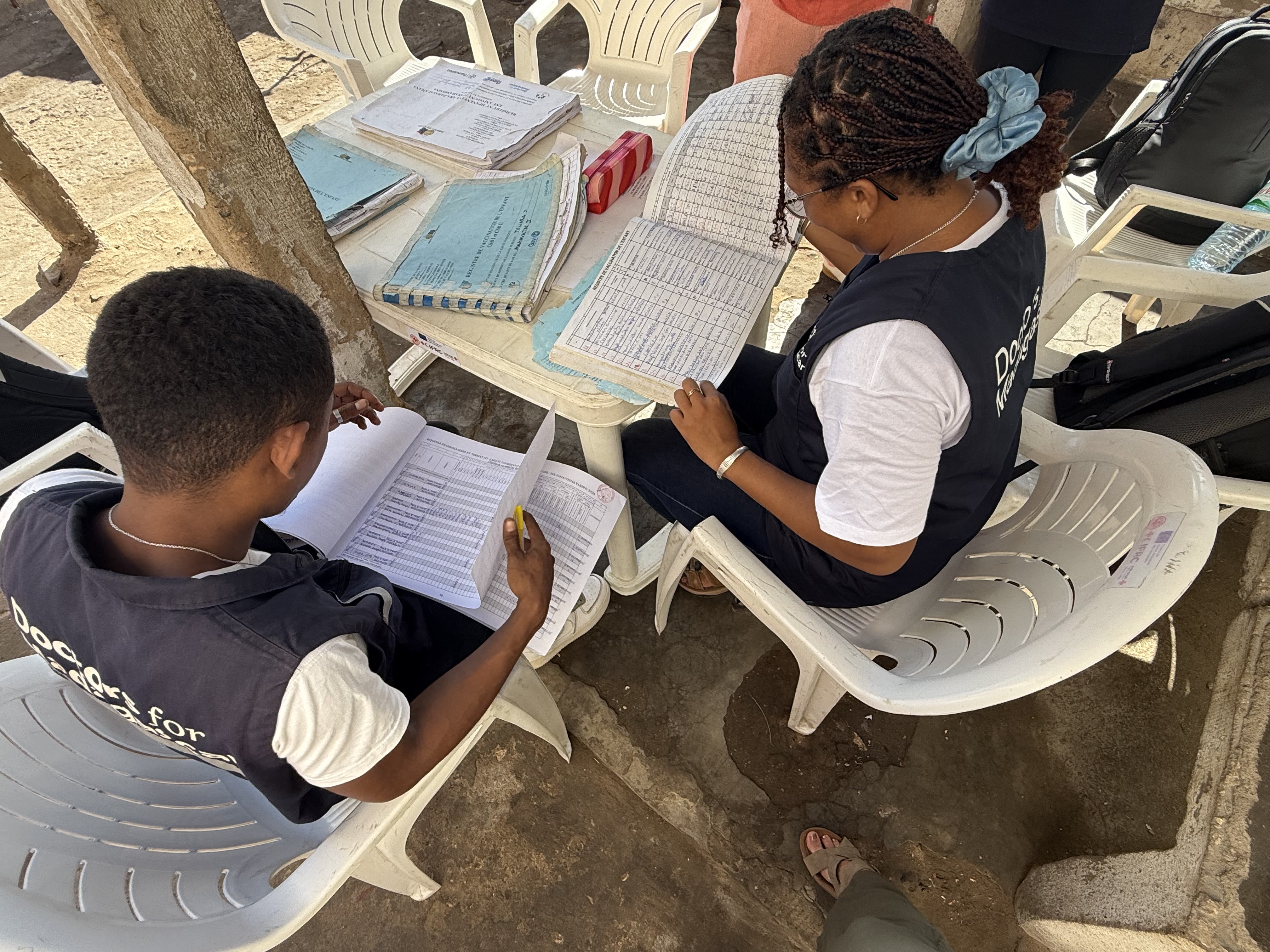
Beyond convincing families to get vaccinated, community health volunteers gather data. They walk around with large booklets, which must be brought into health facilities to cross-check, and that data is funneled up to the central government, telling them where areas of low immunization are.

On a recent afternoon, Doctors for Madagascar spent hours training four community health volunteers on filling in vaccination books at the Bemanga clinic. The organization has mapped out zero-dose children and is working to ensure they’re vaccinated in 16 priority districts in the south.
The volunteers learn things such as estimating birth dates, as some parents don’t know them. They chat with parents about how many harvests have passed as an estimate. They also learn how to draw chalk marks on doors.
After the training, the volunteers walked to a neighboring village. At the second house they visited, they found an 8-month-old child who was vaccinated during last October’s polio campaign, but the mother hadn’t brought the child in for the second dose. She said the clinic was too far, yet they live practically a stone’s throw away.

This underscores another challenge: Vaccinations aren’t always a family’s priority in a country with high poverty levels. Visiting a clinic may come at the cost of a day’s wages.
And despite the critical work they do, community health volunteers across the country are not paid. And while many have personal reasons for supporting their community, it also means they, too, must choose priorities.
Ravaonindrina Antoinette, a community health volunteer, said she sometimes walks an hour and a half to reach a community, only to find that some families aren’t home. That’s difficult, when she also has to manage feeding her family.

Beyond this, there are security risks, including bandits in some parts, making travel unsafe.
Organizations support volunteers in a patchwork of ways. This means support varies: from a monthly stipend or a payment for referring a child for vaccination, to compensation for community mapping, or a daily allowance during a polio campaign.
One issue, though, is that organizations aren’t equally spread across Madagascar — some districts have many, while others have hardly any.
America’s withdrawal


For over 30 years, the U.S. Agency for International Development has been a leading health donor in Madagascar. But that was brought to a halt under the Trump administration.
But the ghosts of the U.S.’ imprint still linger. Plastered on the walls of health clinics across the country are posters for USAID’s ACCESS program, and community health volunteers still wear clothes with the program’s logo.

Implemented by Management Sciences for Health and its partners, ACCESS used to support over 20,000 community health volunteers to provide broader primary health care services, including vaccine promotion and referrals. Many received smartphones, tablets, and bicycles. It also supported polio campaigns and transported vaccines to facilities across 60 districts.





One focus was improving data — digitizing it and making it accessible to decision-makers. Community health volunteers were provided reimbursements for the distance traveled and accommodation to come to meetings where data was consolidated, including on vaccinations.
This phase of the program was winding down this year, but the Trump administration’s dismantling of USAID brought the remaining work to a halt in January.
Before Trump took office, there were expectations the work would continue — there’d been a call for proposals for the program’s next iteration.
But projects such as ACCESS aren’t in line with the Trump administration’s vision, which includes deprioritizing “broad and stand alone behavior change, health systems strengthening, knowledge management, broad research, and technical assistance.”
And there are no signs that ACCESS will return.








A health facility chief said that since the program ended, the number of patients referred to her clinic has decreased, and so has data quality.
Some health volunteers are no longer spending time visiting villages and coming for monthly meetings to cross-check data because they no longer receive cost reimbursements.
Other terminated USAID Madagascar programs could also stem efforts to keep polio at bay, such as a $35 million project launched last year to improve clean water access and sanitation in rural areas; a $10 million sanitation project in urban areas; and a $1.3 million WHO grant aimed at supporting health systems, strengthening mental health services, and enhancing disease outbreak response.
Beyond USAID, the U.S. told Gavi it’s cutting its support. The country also announced its withdrawal from WHO and has proposed UNICEF funding cuts.
The GPEI said U.S. funding cuts haven’t materially affected their own budget this year, and the U.S. budget process is ongoing, but they are expecting a decision on future polio funding from the U.S. in the coming months.
The biggest immediate gaps have been with the U.S. CDC’s activities, particularly surveillance. Countries across Africa have had to reduce the frequency of collecting samples from the environment to test for the poliovirus and halt expansions in high-risk areas, according to the initiative.
“Overall, the GPEI is preparing for significant cuts from some of its biggest donors that will force the program to make tough decisions very soon,” the initiative told Devex.
But there’s also been a delay in the processing of samples already collected. This has led to several new accreditations for African labs to process samples themselves — something that has been in the works for years but has been accelerated.
Some sources said they hope decreased foreign aid will make the Malagasy government less dependent on donors, but they’re also concerned it doesn’t have the resources to cover shortfalls.





“Ultimately, achieving and sustaining polio eradication is only possible when all health partners (civil society organizations, essential immunization programs) have the resources they need to ensure every child is protected through vaccines,” GPEI said.
But despite diminished resources, there have been global calls for sustained prioritization of vaccines, as one of the most cost-effective public health interventions. According to UNICEF, one vial of oral polio vaccine costs $2.82 and contains 20 doses.
“The idea of a child dying or being paralyzed by a vaccine-preventable disease is just tragic,” Gavi’s Clark said.
“It’s critical that children are given the same opportunities in Madagascar as they’re given in Manhattan.”
“It’s the responsibility of the world to take care of its children,” she added.
Editor’s note: This story was supported by a U.N. Foundation press fellowship. Devex retains full editorial independence.
Photos by: Sara Jerving
Copy edited by: Florence Williams, Nicole Tablizo, and Sheri-kae McLeod
Produced by: Mariane Samson