
Local action for global impact: Making shorter TB preventive treatments more accessible for all
Tuberculosis is one of the leading causes of death worldwide, especially among people living with HIV, but short-course preventive treatments are now more affordable and available, thanks to a locally led consortium working to expand access globally.


Stanley Sibanda was diagnosed with HIV in 2006 while he accompanied his sick uncle to Mpilo Central Hospital in Bulawayo, southwest Zimbabwe. After noticing a skin rash on Sibanda’s face, the doctor advised him, “If I were you, I would be tested for HIV right away because the symptoms you have are concerning,” he recalled.
Initially, Sibanda was reluctant to take an HIV test, and after receiving a positive diagnosis and starting his treatment, the fear of stigma and discrimination prevented him from disclosing his status to others, he said.
In 2016, Sibanda was offered tuberculosis preventive treatment, or TPT, which had been introduced in Zimbabwe a few years prior. But once again, social stigma held him back from taking the medication. “At first I refused to take it because of beliefs and misconceptions about how those pills could cause TB or burn your skin,” he said.
Sibanda did eventually begin taking TPT — but his experience represents a broader struggle in Zimbabwe, where both TB and HIV remain serious public health concerns, with stigma, discrimination, myths, and misconceptions surrounding them.


Overcoming the barriers to accessing TB preventive treatment


Tuberculosis is the leading cause of death among people living with HIV, who are 18 times more likely to develop active TB disease than people without HIV. Globally, TB killed 1.3 million individuals in 2022, including 167,000 HIV patients. TB preventive treatments are urgently needed since people living with HIV and household contacts of TB patients, particularly young children under 5, are more likely to get active TB.
TPT has been shown to be successful in preventing the onset of active tuberculosis, with an efficacy rate ranging from 60% to 90%. The World Health Organization’s End TB strategy aims to reduce global TB incidence by 80%, TB deaths by 90%, and to eliminate catastrophic costs for TB-affected households by 2030 — but the targets cannot be met without increasing the use of TPT.
Until recently, the standard for TPT consisted of a daily dose of an antibiotic called isoniazid — known as IPT, or isoniazid preventive therapy — typically taken for six, nine, 12, or 36 months. Due to the length of treatment and the high pill burden, it has had limited acceptance and low patient adherence since it was established nearly 60 years ago.
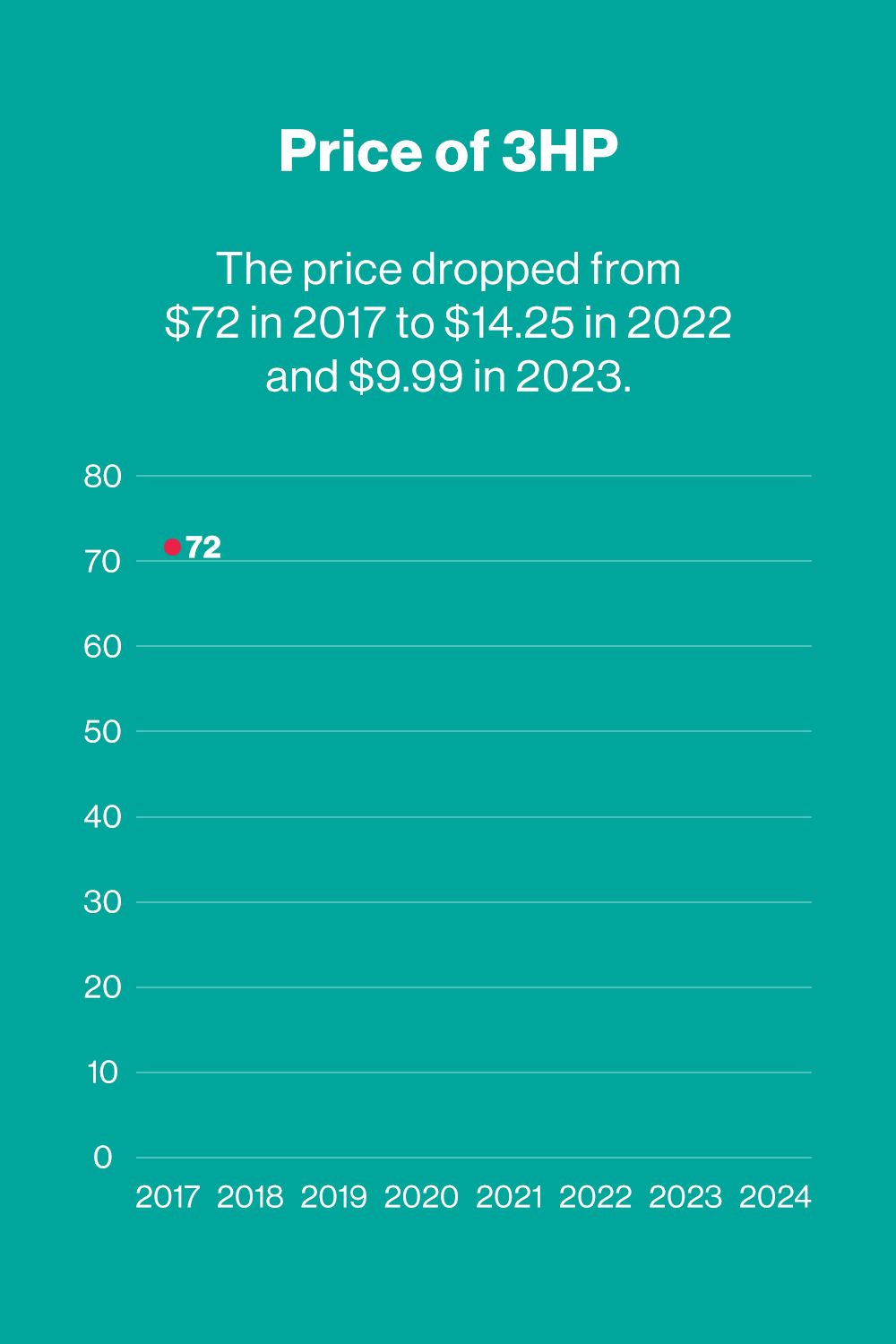
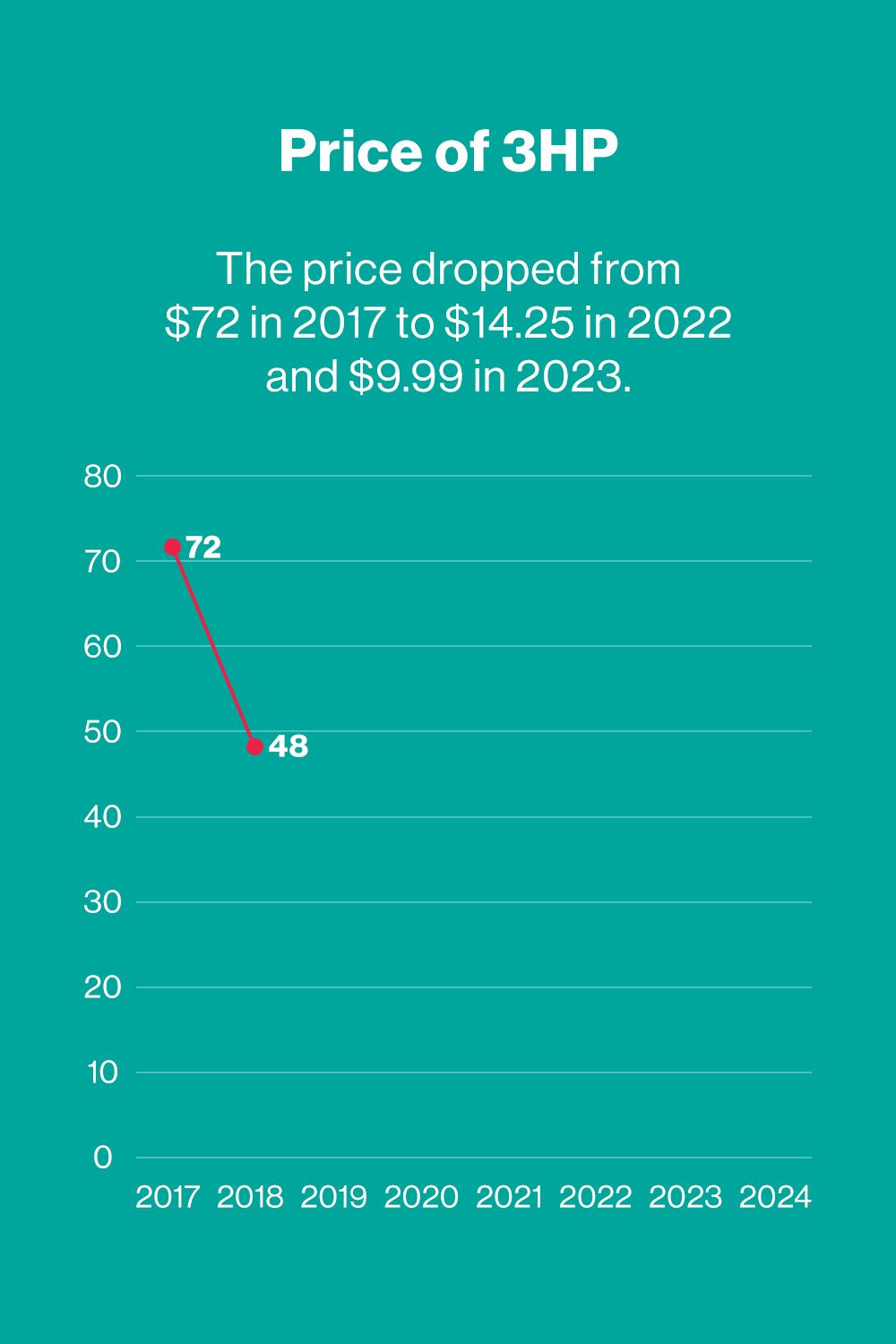
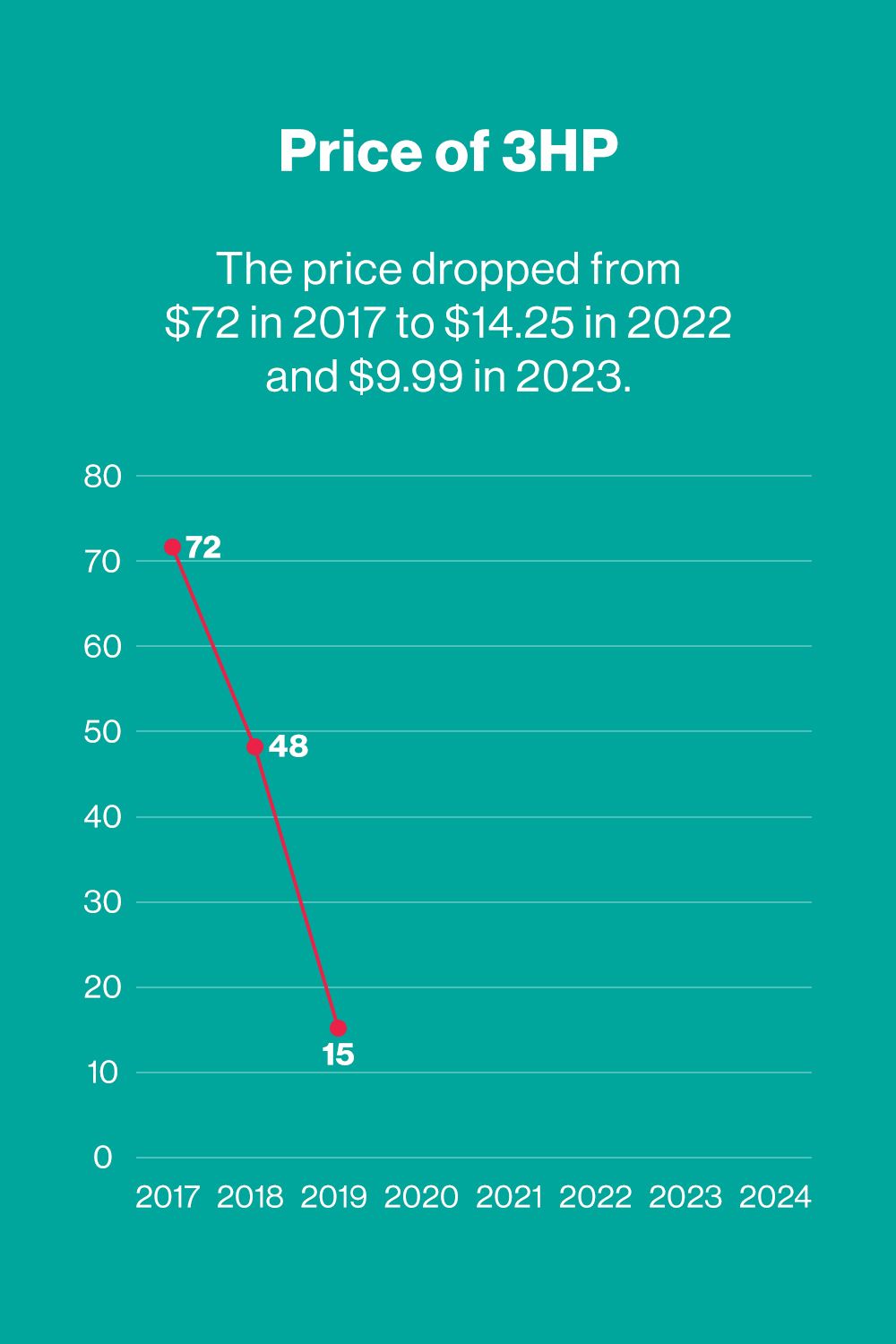
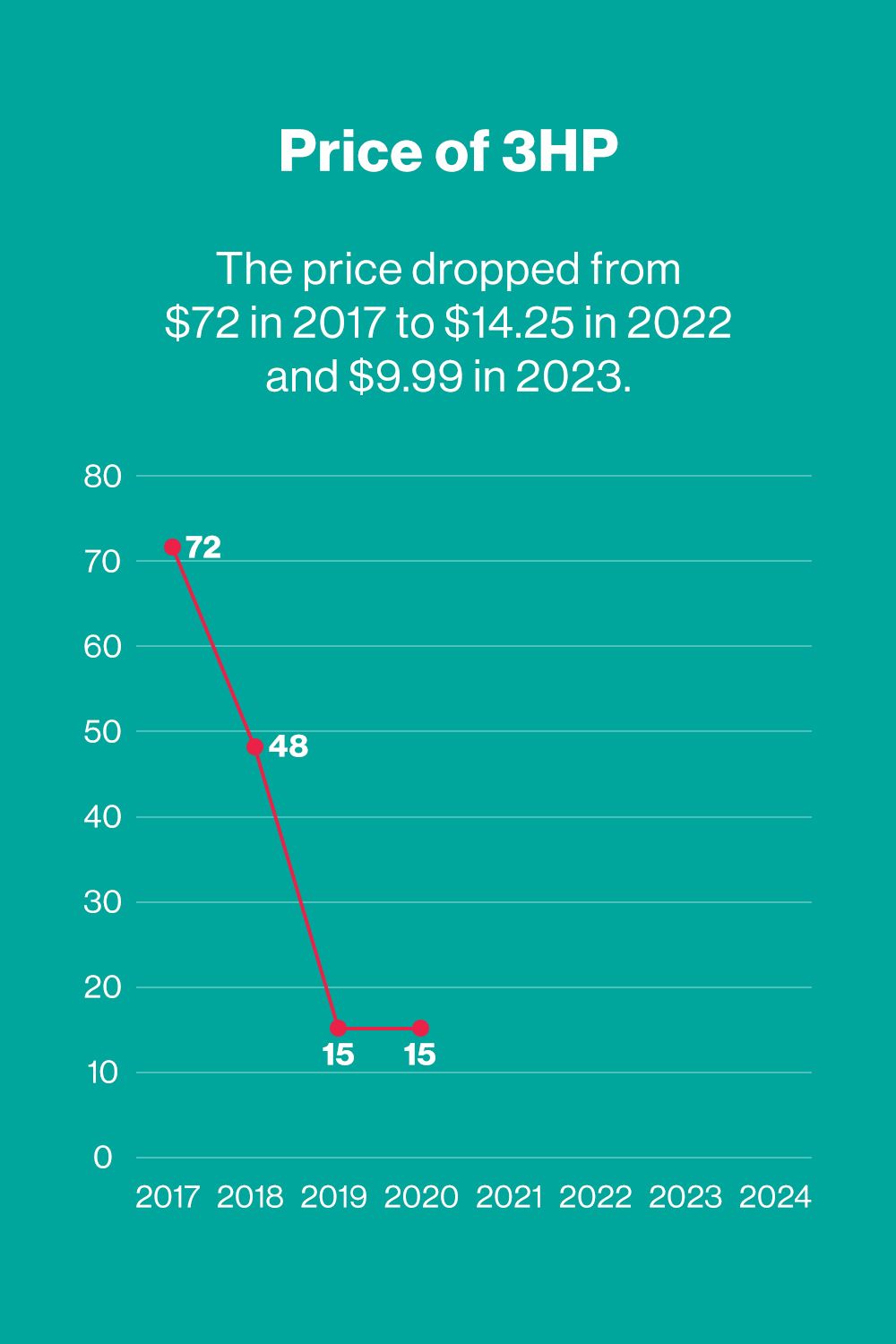
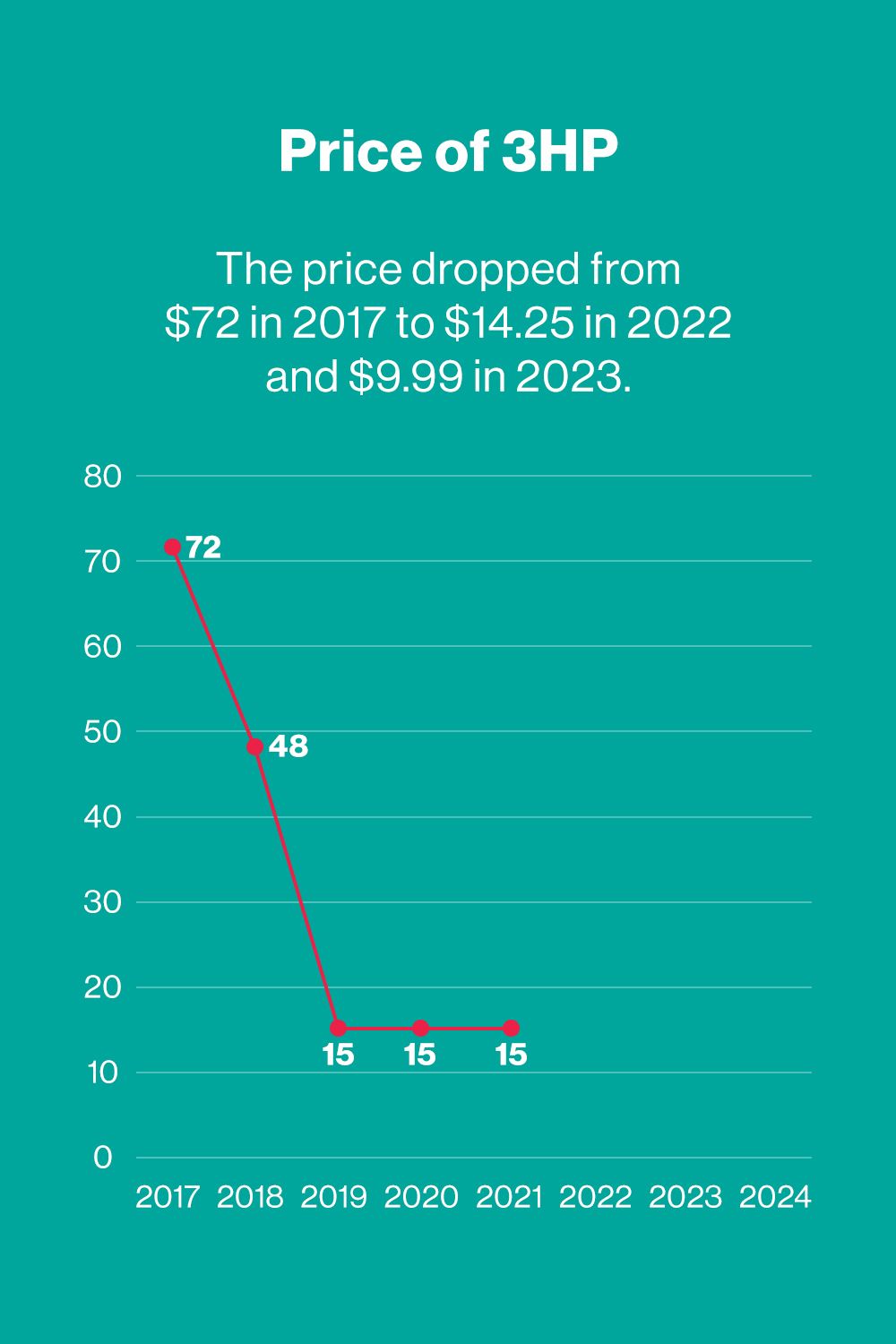
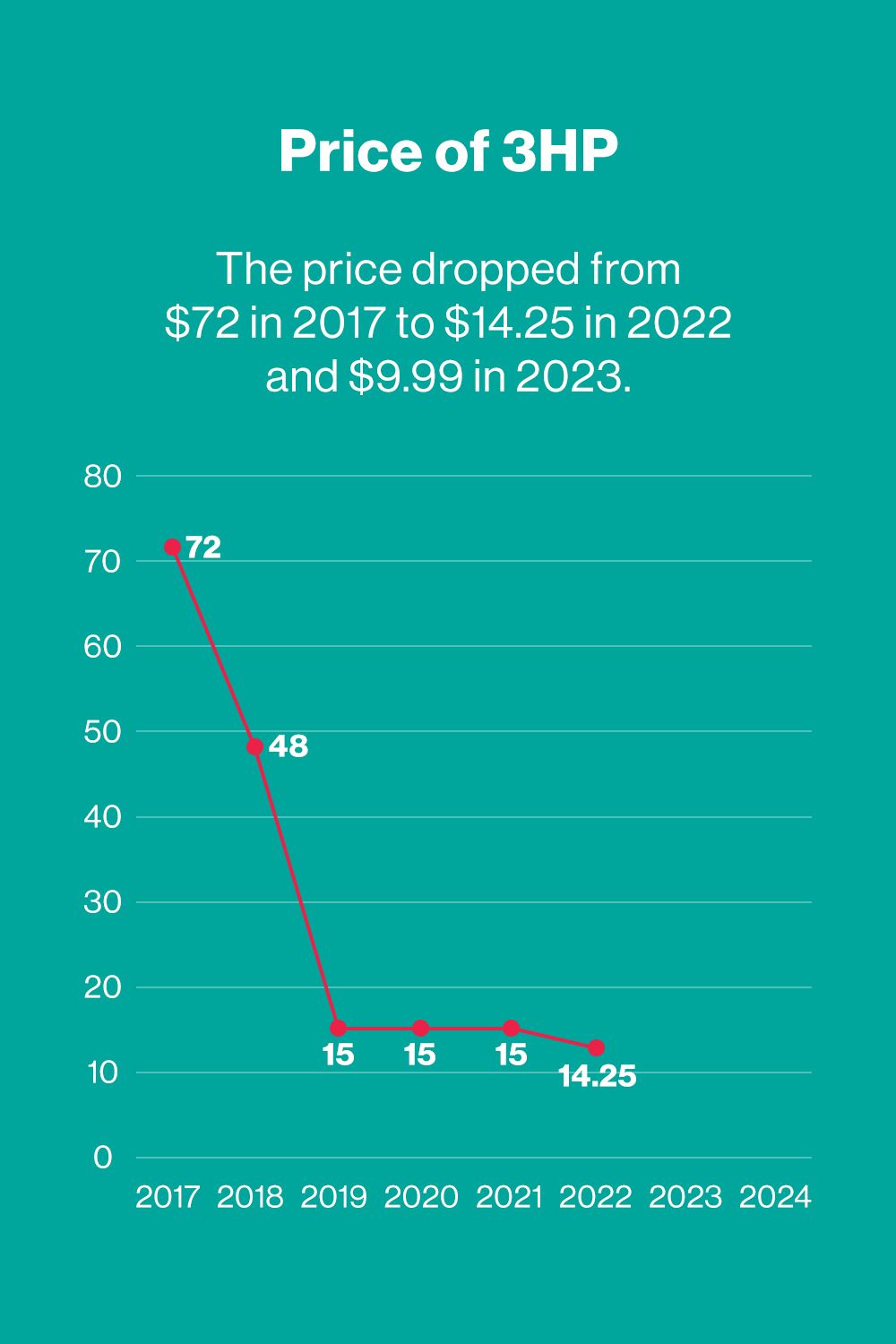
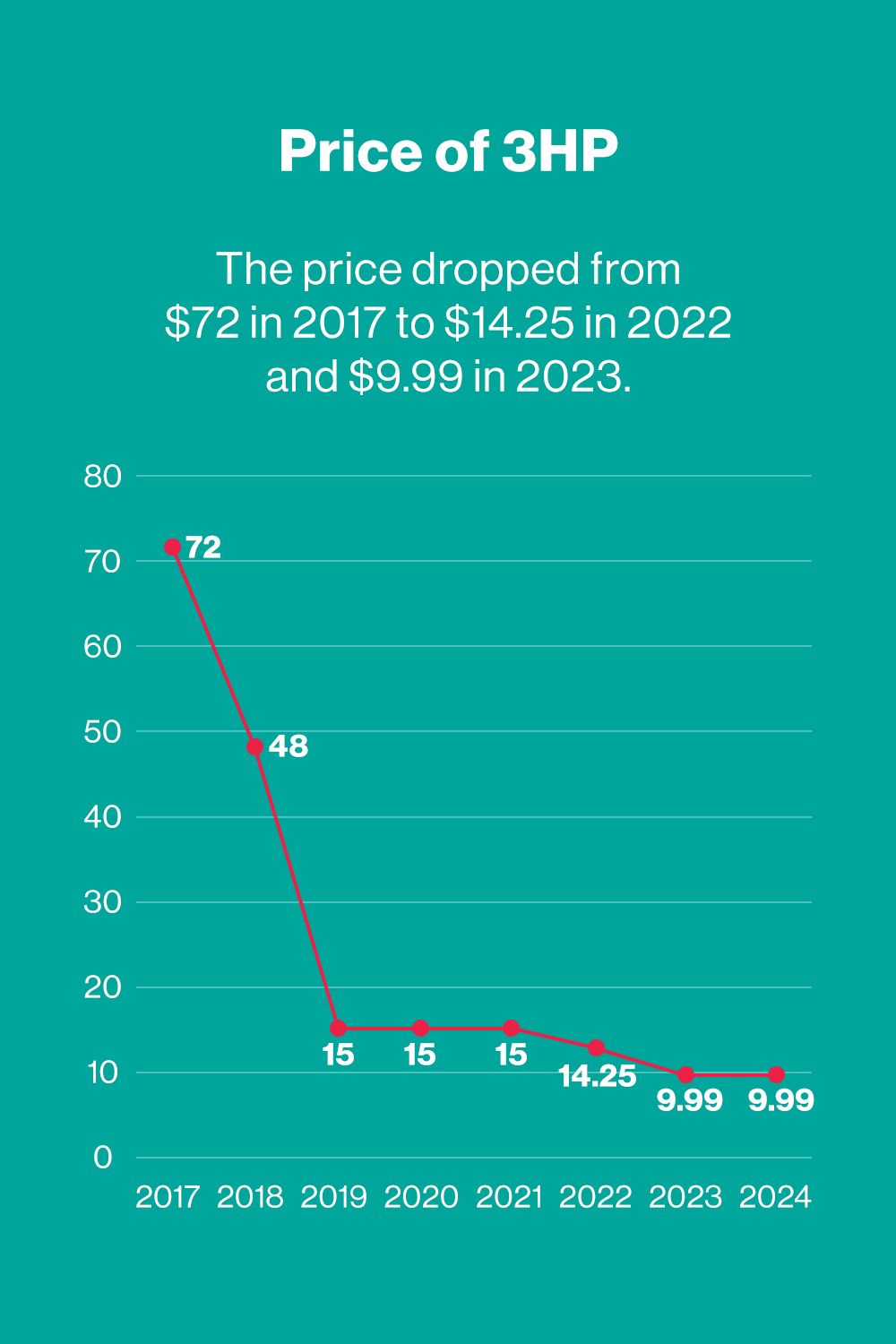
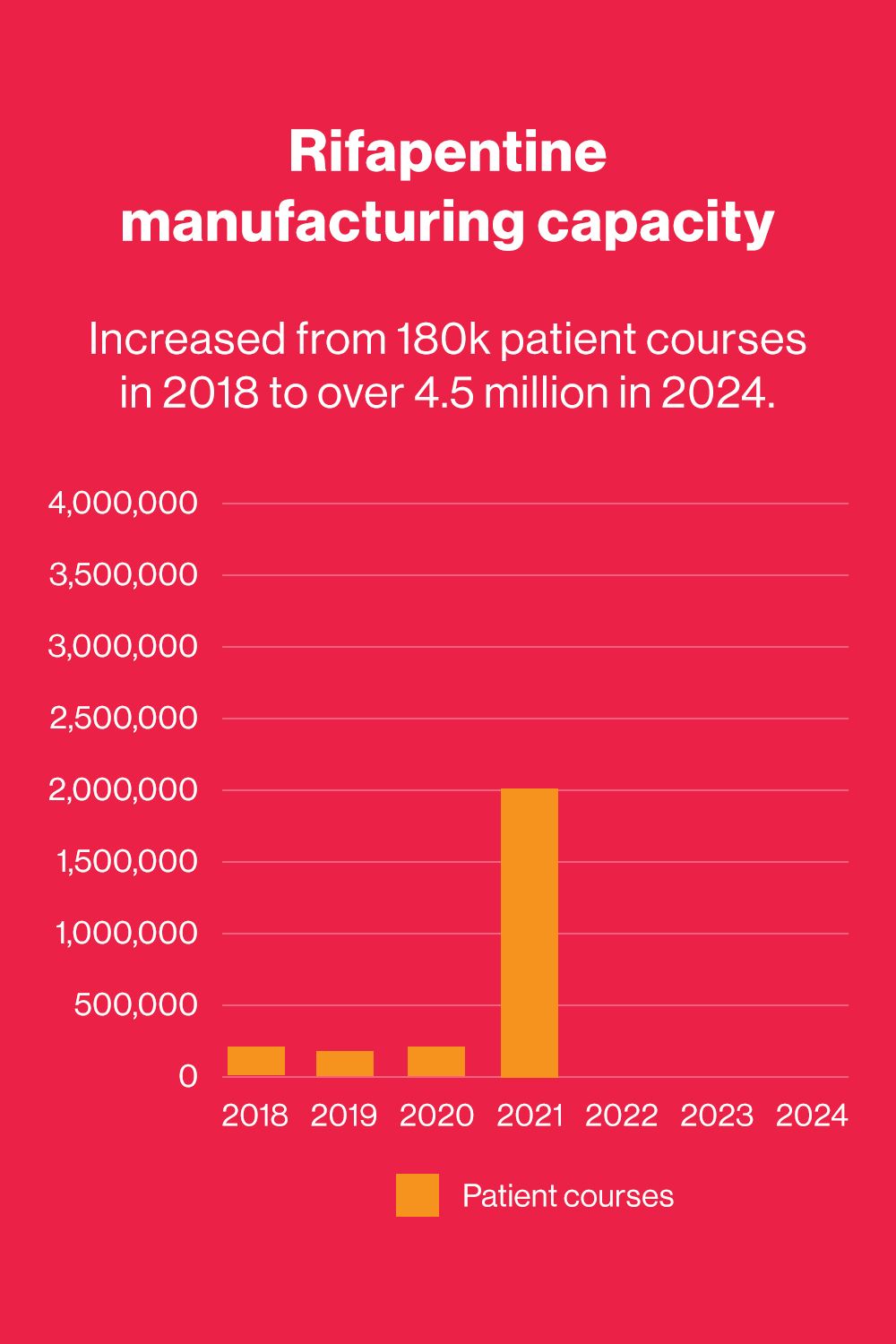
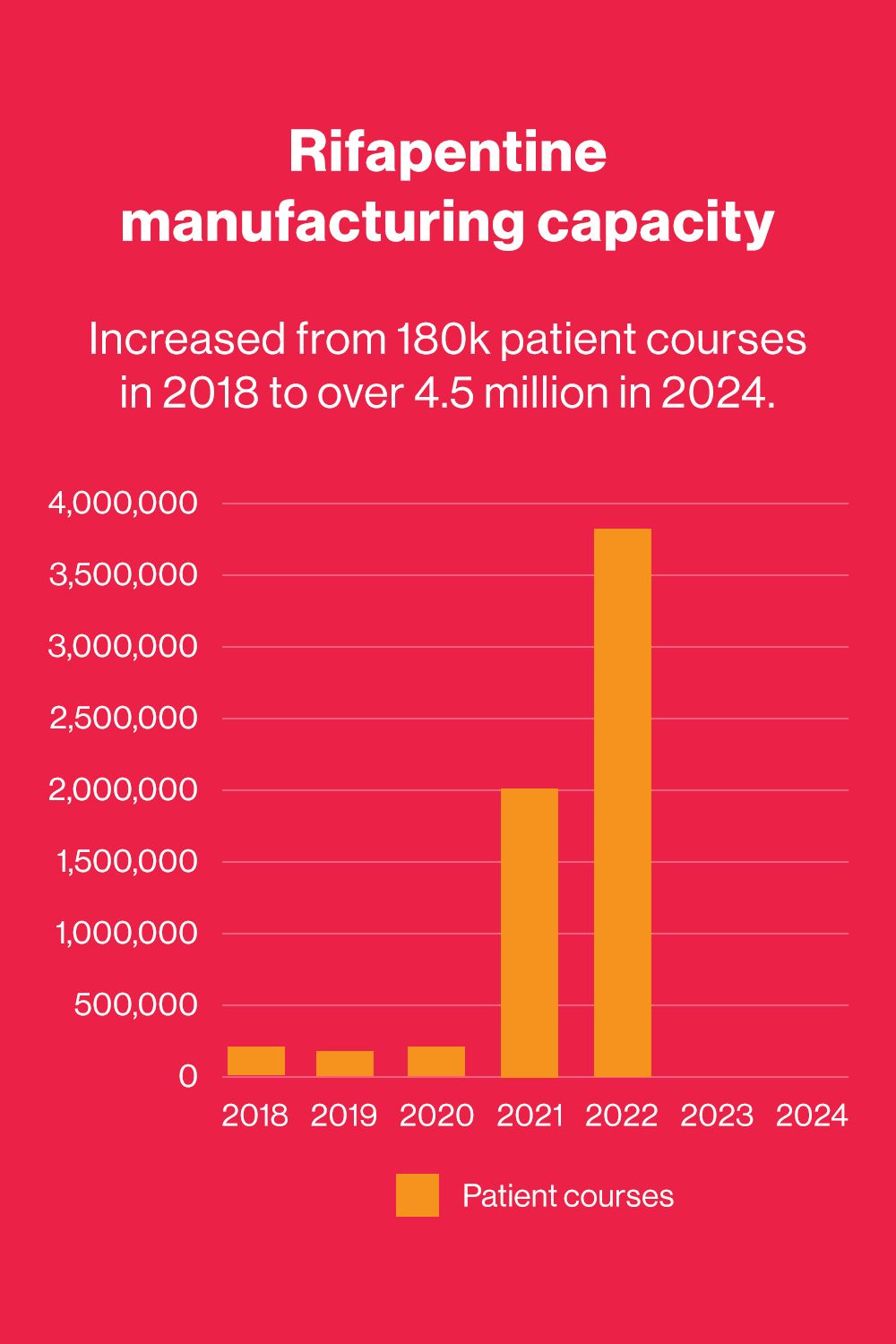
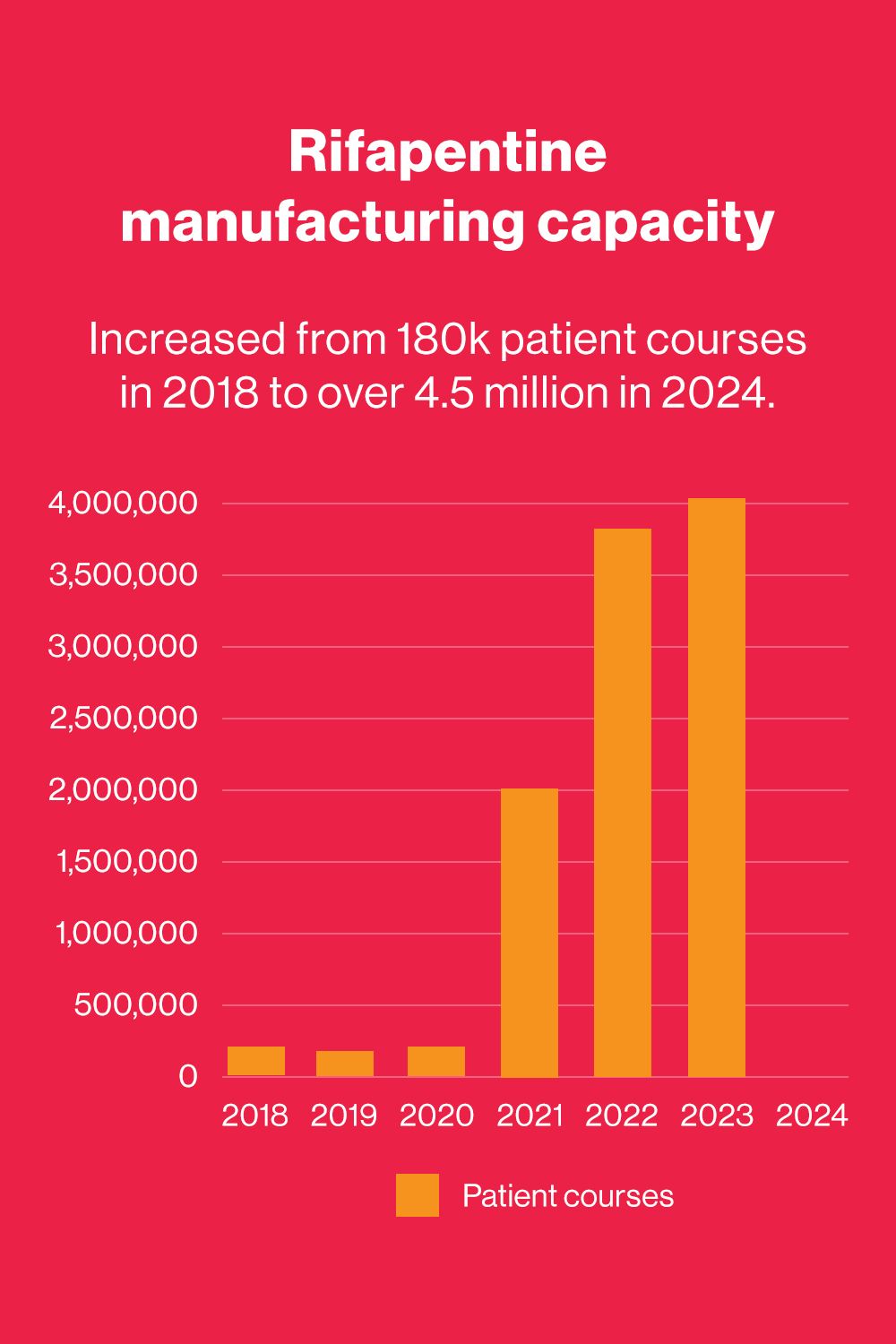
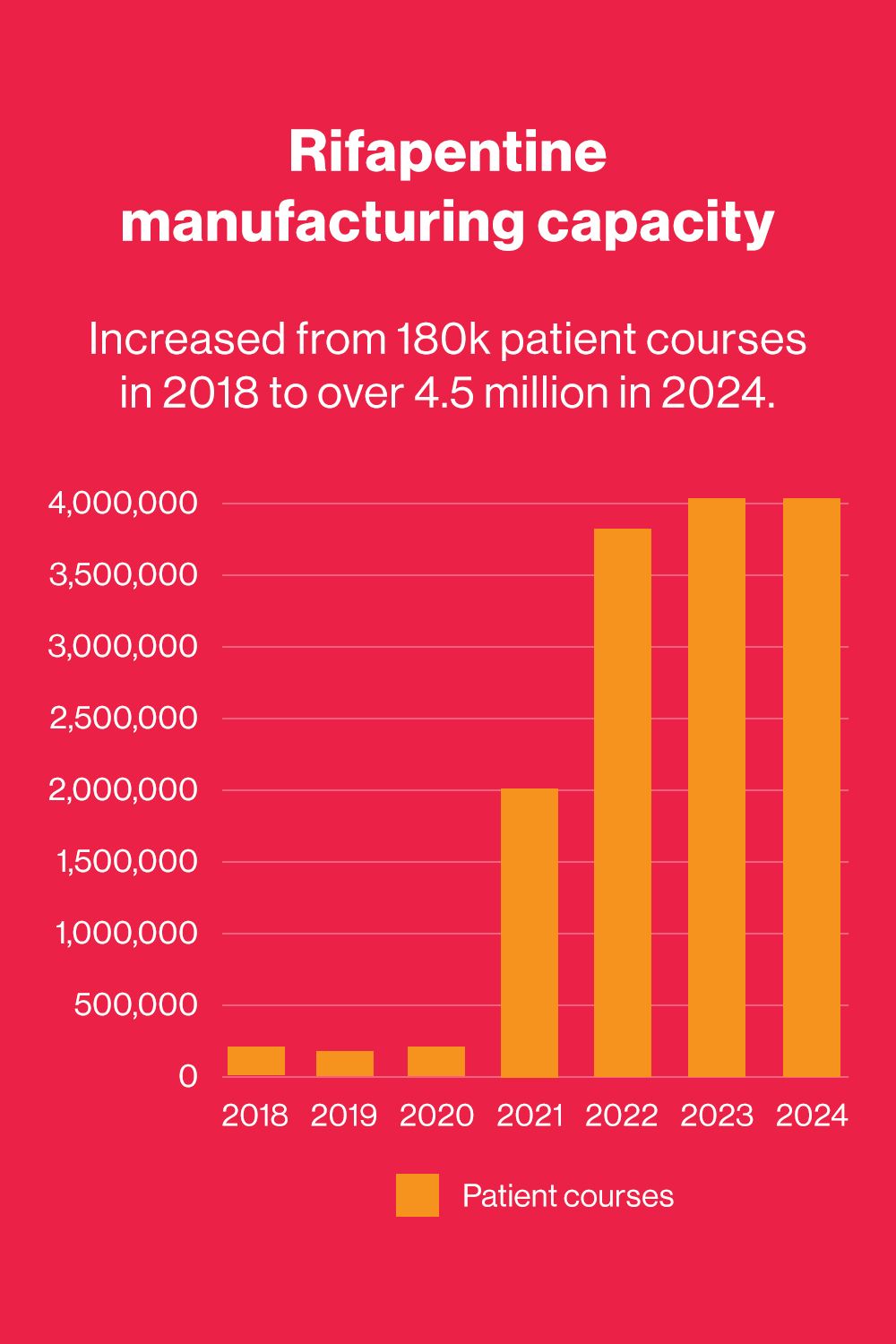
A shorter treatment regimen exists, known as 3HP — a fixed-dose combination therapy that combines two antibiotics, isoniazid and rifapentine, taken once a week for three months. But until relatively recently, it was only available from one supplier, Sanofi, at a cost of $72 per treatment course, and therefore was mainly used in the United States. “The challenge was it wasn't produced in sufficient quantities, and the price was substantially more than the other standard of care [IPT],” said Robert Matiru, director of programs at Unitaid.
“Not even the donors supporting these low- and middle-income countries were willing to pay that much,” said Makaita Gombe, market access director at The Aurum Institute, a leading Africa-based global health organization, which leads IMPAACT4TB, a consortium working in collaboration with WHO and funded by Unitaid.


Making short-term TB preventive treatments accessible


Following a call for proposals from Unitaid to address the lack of safe, affordable, and accessible short-term TPT, IMPAACT4TB was launched in 2017. “I think the whole world had realized that we needed a way to prevent TB that was not as long as the regimen that was there at that time,” Gombe said.
Drug to drug interactions were a concern, and research was first needed on the safety of co-administering antiretrovirals, or ARVs, and TB preventive medications, including modifying the formulation to increase demand: fewer pills, easier pill packs, lower prices, and a single pack of pills in blisters for weekly dosing, Gombe said.
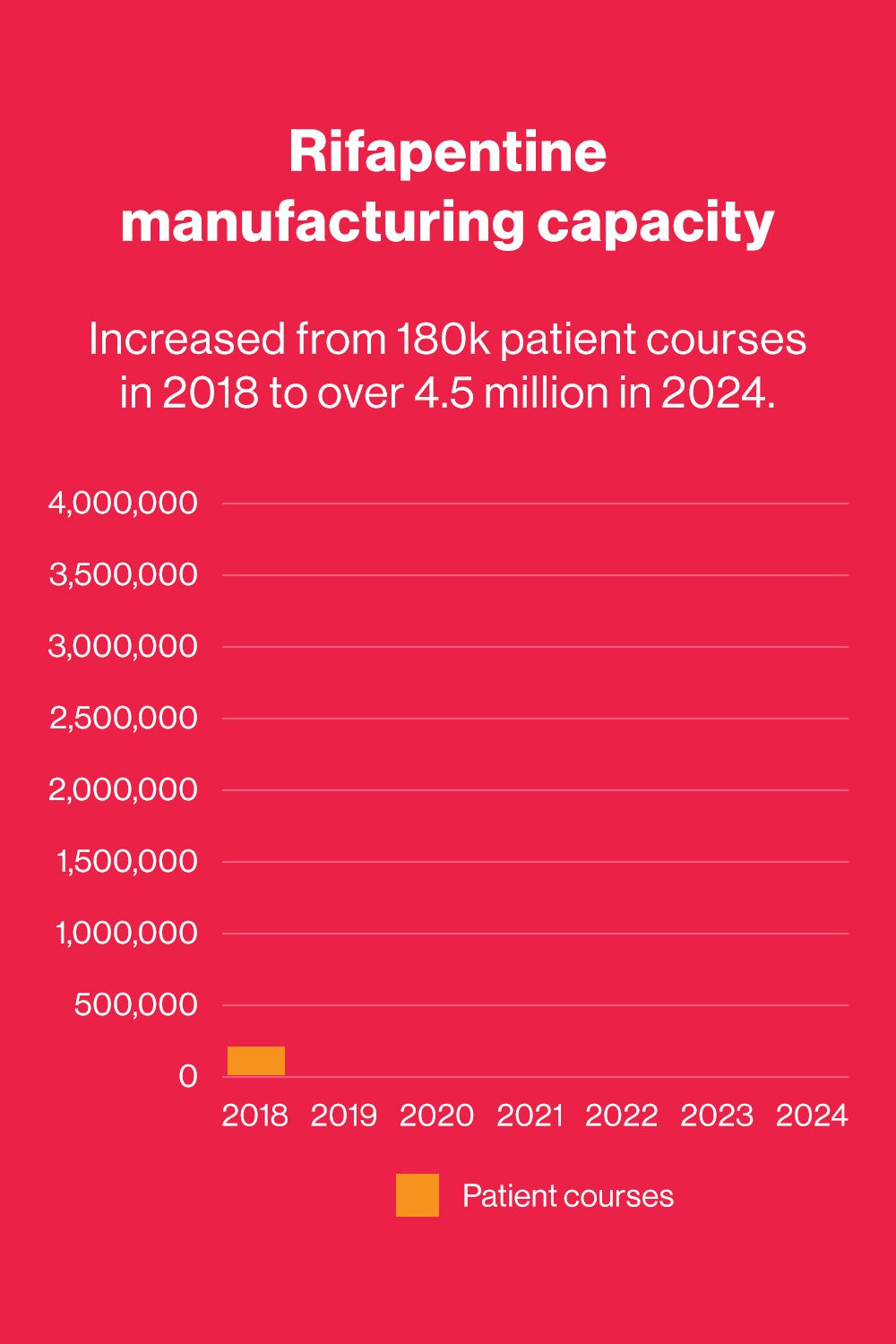
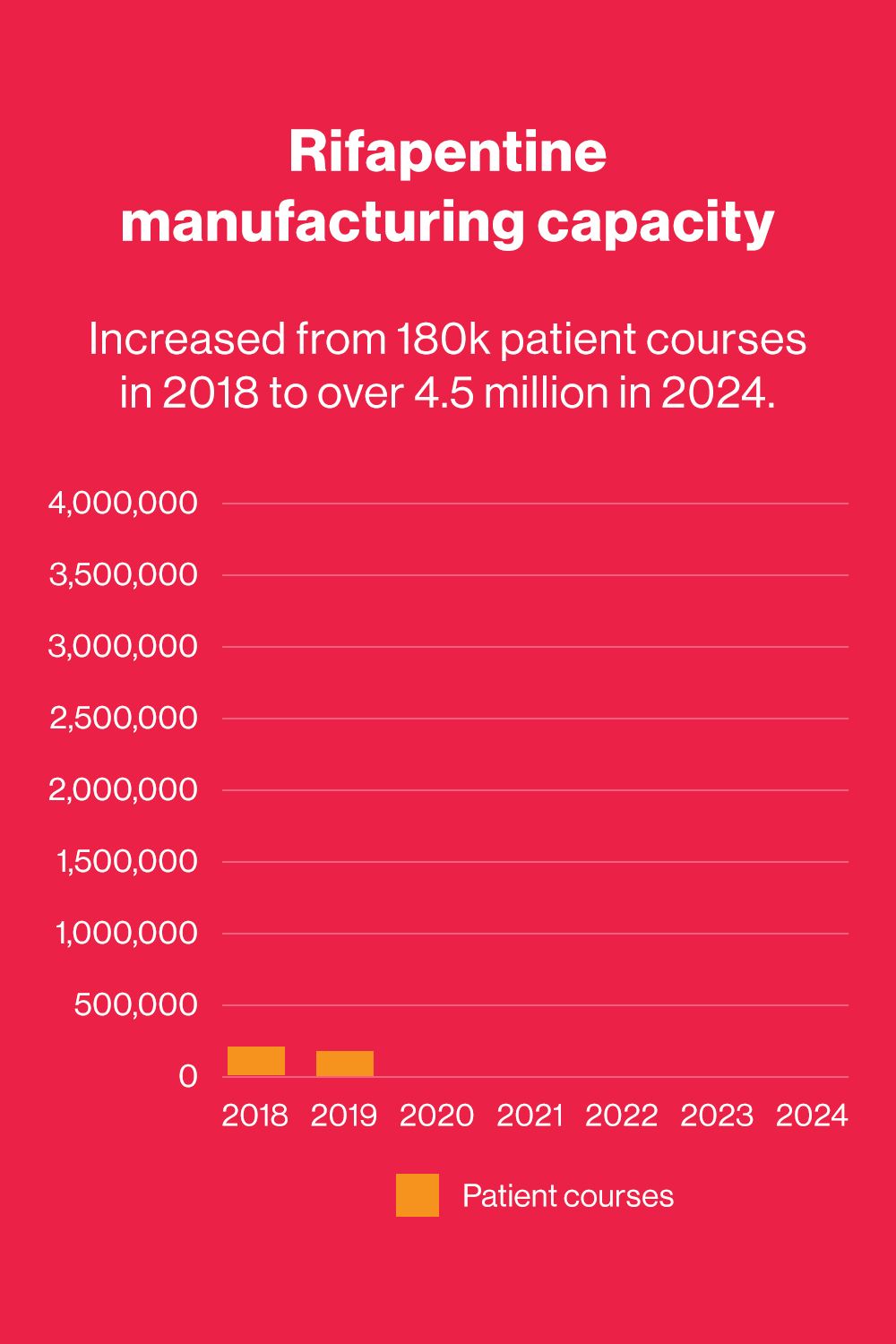
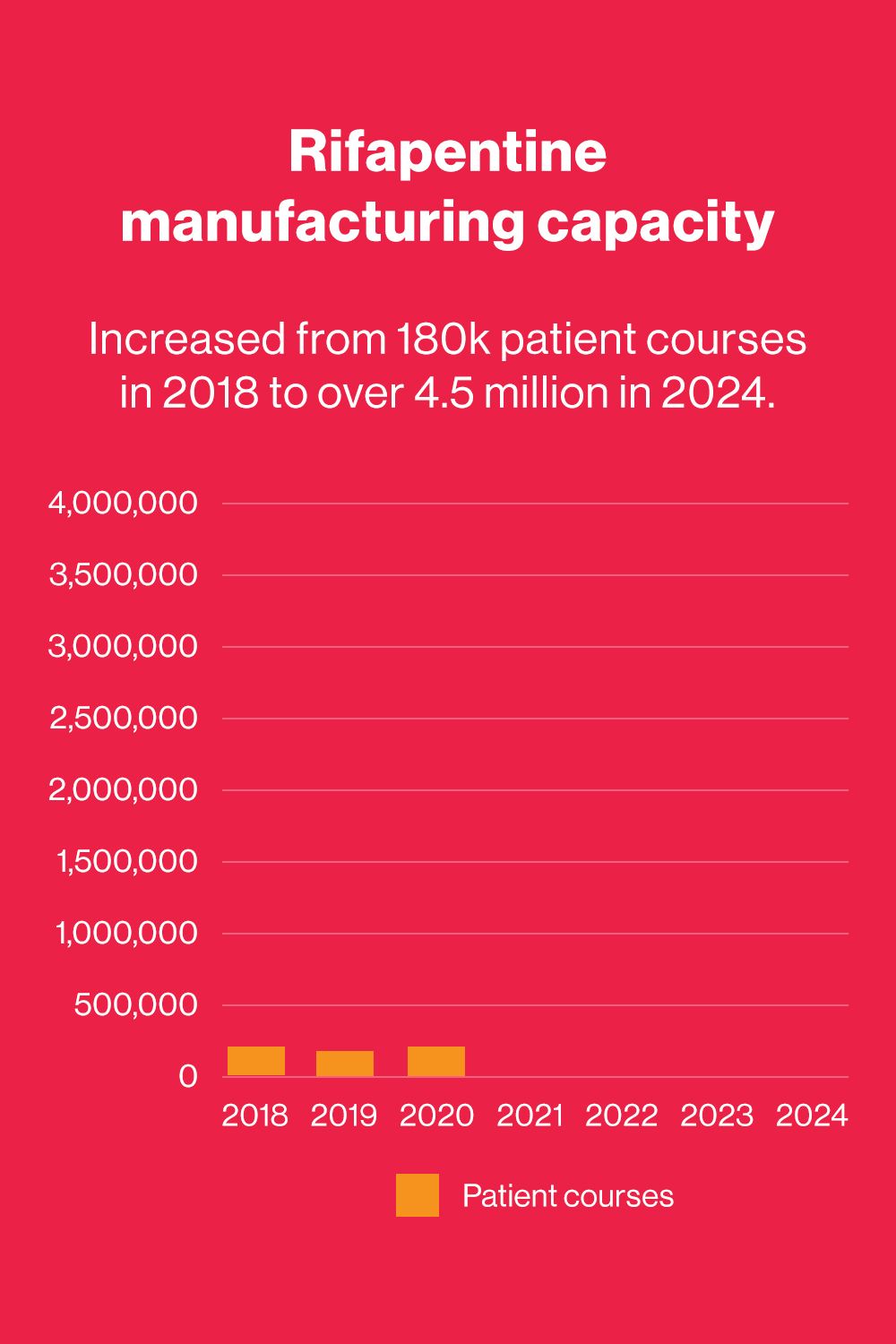
In addition, Aurum, Unitaid, and IMPAACT4TB consortium member Clinton Health Access Initiative brokered a deal that allowed two generic manufacturers, Lupin Limited and Macleods Pharmaceuticals, to introduce formulations of rifapentine at competitive prices, lowering the price per patient course from $72 to $10. The consortium also worked with manufacturers to bring the treatment regimen down from an initial nine pills to a three-pill regimen, including the development of a monthlong regimen known as 1HP.


Makaita Gombe, market access director at The Aurum Institute
Makaita Gombe, market access director at The Aurum Institute
Shorter medication regimens significantly increase the likelihood that a patient will finish their term of TPT, resulting in better outcomes and more lives saved. “This shorter regimen is very fair to us because of the pill burden,” said Sibanda. “Patients can select to get one box of TPT course to take with their ARVs, eliminating the need to return to the clinic,” Gombe added.
The impacts of the initiative are not only being felt in lower-income countries. So far, more than 78 countries around the world have purchased 3HP at a lowered price of $10 per patient course. “To us, this is a testament of people who need the product actually being able to access it. And really, that's because of evidence generated for use in broad populations, innovations in service delivery, the different formulations, and the price,” Gombe said.
Addressing Zimbabwe’s TB burden


Zimbabwe is one of the top 30 countries when it comes to TB and HIV burden, where people suffer both TB and HIV at the same time. Of those identified as having TB disease, about 51% are found to also have HIV, according to Dr. Manners Ncube, the national TB and HIV technical officer in Zimbabwe’s Ministry of Health and Child Care.
Dr. Manners Ncube, the national TB and HIV technical officer in Zimbabwe’s Ministry of Health and Child Care, outlines what more needs to be done to address the country's TB burden.
Some 33,000 new cases of TB were recorded in Zimbabwe in 2022 — a rise from about 30,000 cases in 2021. While progress has been made over the past decade, the country still grapples with nearly 15,000 missed TB cases annually and a high burden of drug-resistant TB.
“Control measures have been working quite well, but starting in 2019 we found out that we are finding fewer cases of TB against the estimates,” Ncube said. The COVID-19 pandemic led to a decline in TB notifications and disrupted availability of health services across the country, he added.


Laboratory medical microscopist Junior Banguza prepares TB patient samples for analysis at Rujeko clinic in Harare.
Laboratory medical microscopist Junior Banguza prepares TB patient samples for analysis at Rujeko clinic in Harare.

A GeneXpert sample is prepared for analysis.
A GeneXpert sample is prepared for analysis.

Junior Banguza uses a GeneXpert machine to prepare a tuberculosis diagnosis in the laboratory.
Junior Banguza uses a GeneXpert machine to prepare a tuberculosis diagnosis in the laboratory.
Raising awareness about TPT through community-led organizations


Community organizations play a crucial role in finding missing TB cases — and their involvement in the IMPAACT4TB consortium is a key strength of the initiative, according to Matiru. “[Aurum] came with strong partners, including a strong community and civil society engagement piece,” he said. This included working with consortium partner Treatment Action Group to make targeted awards to community-based networks in each of the implementing countries to help with demand generation and socialization around the uptake of 3HP.
Jointed Hands Welfare Organization's Melody Mukundwi discusses why awareness raising and demand generation for 3HP is important for tackling the spread of TB.
In Zimbabwe, Jointed Hands Welfare Organization is one of the local organizations working to raise awareness and demand for 3HP, including working with the government on revising national TB guidelines.
“The challenges that we see in the communities that we work in mostly revolve around issues of limited information and knowledge about TB preventive therapy,” said Melody Mukundwi, resource mobilization and communication liaison officer for Jointed Hands Welfare.
“Expert patient” Stanley Sibanda talks about what it means for him to be involved in community outreach around uptake of 3HP.
The organization works with designated “expert patients” like Sibanda — who now leads the Zimbabwe National Network of TB Survivors — to push awareness campaigns, including contact tracing in communities where they live. “We are giving awareness through social media, radio stations, and television networks,” Sibanda said.




In Sanyati district, which has a TB/HIV co-infection rate of 67% — 13 percentage points above the national average — Tendayi Westerhof, director of the PAN-African Positive Women's Coalition Zimbabwe, has been running a project to create demand for TPT for children and other household contacts.
Tendayi Westerhof, director of PAN-African Positive Women's Coalition Zimbabwe, discusses what goes into the training of village health workers on TPT.
“We have trained village health workers on TPT. We have also held community dialogues with community leaders in Sanyati district, mostly TB survivors and mothers who have had children who have been affected by TB, including health care workers,” said Westerhof, who herself was diagnosed with HIV 23 years ago.
“As the community, we are not only the recipients of services but we know the culture, the way of living of people on the ground, and how they react when new information comes,” Westerhof said. “Our role really is to make sure that these policies are user-friendly and they make TB preventive treatment accessible to everyone who needs it.”
This model was the same in 12 countries where demand for TPT was generated from the affected communities, forming a movement of global activists trained in the science of TPT.
The road ahead


To make progress in the fight against TB in countries like Zimbabwe, community awareness must be strengthened further, Ncube said. “TB is more than just a disease of a person; it is a community disease. So there are some factors that affect someone ending up with TB, [or] someone successfully being treated for TB, that are beyond just the Ministry of Health,” he noted.

A community health worker shares information about TPT with patients at Rujeko clinic, Harare.
Local and regional leadership is a key part of the equation, said Gombe — and the IMPAACT4TB initiative is an example of that. “Aurum is based in South Africa. We are part of the people that need this product. South Africa is one of the highest TB burdens alongside India and really this work needs to be done to serve the people around us,” she said.
While a local approach is crucial, Gombe also emphasized the importance of continuous collaboration with global partners. “We work within the communities we serve, but also recognize that we can’t do everything alone. We have global partners that have perfected certain things,” she said, adding that scientists at Aurum partnered with Johns Hopkins University were critical, as were financiers like Unitaid; the U.S. President's Emergency Plan for AIDS Relief; the Global Fund to Fight AIDS, Tuberculosis and Malaria; and USAID, implementing partners like KNCV Tuberculosis Foundation, and pharmaceutical manufacturers.
"It was a united effort, both locally and globally, coming together to create a transformative global movement," Gombe said.
A community health worker shares information about TPT with patients at Rujeko clinic, Harare.
A community health worker shares information about TPT with patients at Rujeko clinic, Harare.
Written & reported by Lungelo Ndhlovu
Edited & produced by Naomi Mihara
Video and photos by Baroque Oeuvre
Video editing and graphics by Mai Ylagan
This piece is sponsored by The Aurum Institute as part of our Roots of Change series. Click here to learn more.

