
Bringing innovation to sickle cell disease patients in sub-Saharan Africa
In Ghana, 15,000 babies are born each year with sickle cell disease. Many go undiagnosed and don’t survive. From Accra, Devex looks at one initiative working to improve access to treatment and care.
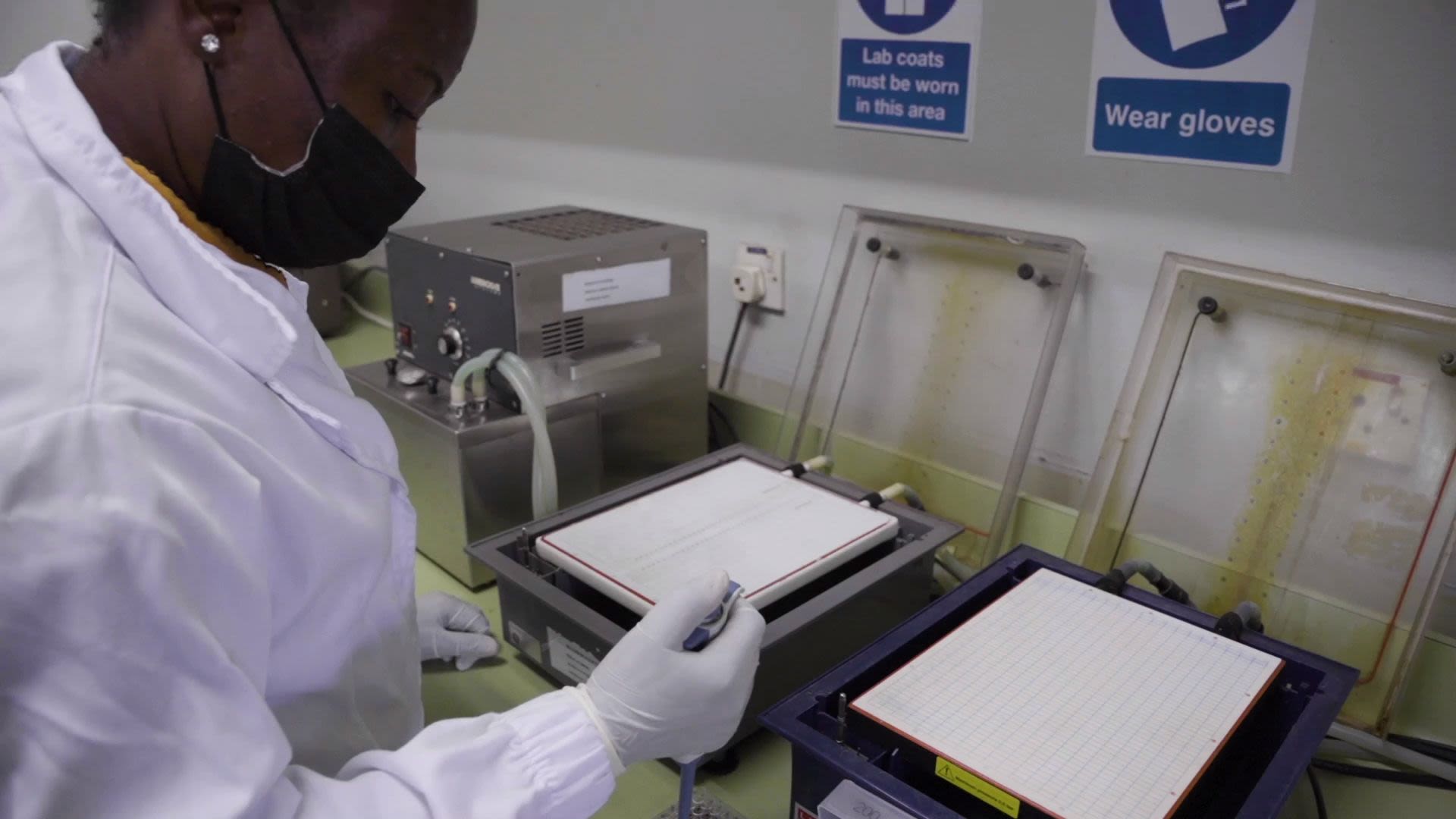
At the Noguchi Memorial Institute for Medical Research in Accra, Ghana, lab scientists screen blood samples of newborn babies in a sickle cell lab. A laboratory shaker oscillates back and forth at one end of the room while a dozen or so scientists clad in white overalls are bent over their workstations. Together they are analyzing the samples to look for the sickle cell gene.
Lab scientists screen blood samples of newborn babies in a sickle cell lab at Noguchi Memorial Institute for Medical Research in Accra, Ghana.
Lab scientists screen blood samples of newborn babies in a sickle cell lab at Noguchi Memorial Institute for Medical Research in Accra, Ghana.
Sickle cell disease is a genetic red blood cell disorder that, if present, can be diagnosed at birth. Unfortunately, this is often not the case in countries with weaker health care systems. While complications and symptoms depend on each individual, lifelong management is usually required to tackle common symptoms such as anemia, ulcers, acute chest syndrome, and recurring pain episodes — caused by the clogging of blood vessels by misshapen red blood cells.

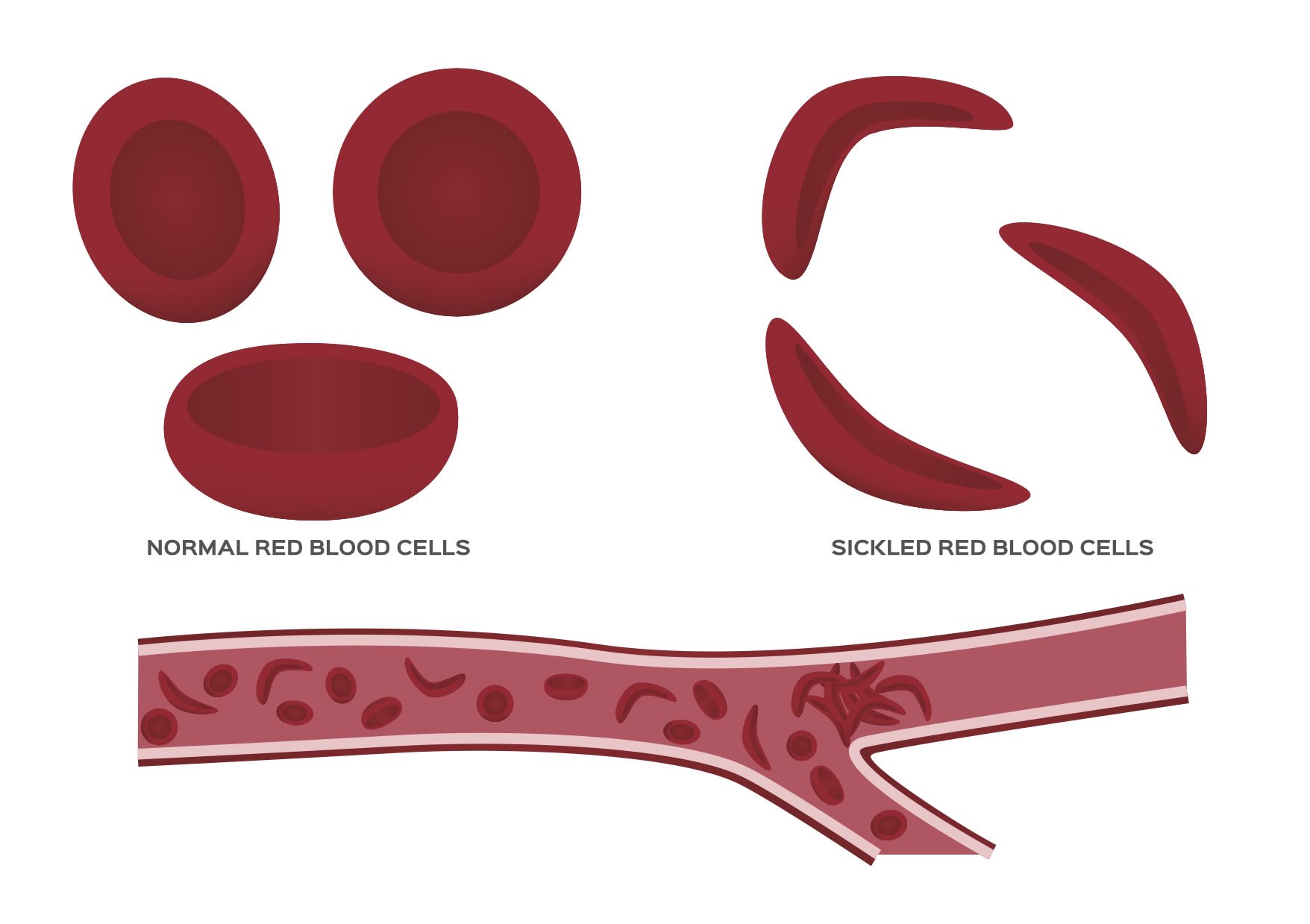
Sickle cell disease causes red blood cells to form a sickle shape, clogging blood vessels.
Sickle cell disease causes red blood cells to form a sickle shape, clogging blood vessels.
According to the World Health Organization, around 5% of people globally are “healthy carriers” of hemoglobin disorders like SCD, but that number rises to 25% in some regions. Of the children born with SCD, 75% to 85% come from Africa.




Dr. Yvonne Dei-Adomakoh, hematologist, analyzes blood samples at Korle Bu Teaching Hospital in Ghana.
Dr. Yvonne Dei-Adomakoh, hematologist, analyzes blood samples at Korle Bu Teaching Hospital in Ghana.
“The burden of SCD in some sub-Saharan countries is of great concern for several reasons. We have got high prevalence of SCD and lack a comprehensive setup for management of these patients,” said Dr. Yvonne Dei-Adomakoh, hematologist at Korle Bu Teaching Hospital in Ghana and senior lecturer at the University of Ghana Medical School.
While the disease can be fatal — the only cure currently available is a bone marrow or stem cell transplant — various treatments to manage the effects of the condition, including the frequent pain crises, exist. Other potential curative treatments like gene therapy are still in early-stage research.
To determine the correct course of action, continuity of care from childhood to adulthood is crucial, and a person’s health status must be reviewed routinely to avoid pain crises or other complications, Dei-Adomakoh explained.
“The earlier you take care of the sickle cell child, the longer this child can live and live a normal lifestyle with a good quality of life,” Dr. Anthony Nsiah-Asare, Ghana’s presidential advisor on health, told Devex. In Ghana, 2%, or 15,000 babies a year, are born with SCD.
According to professor Kwaku Ohene-Frempong, president at the Sickle Cell Foundation of Ghana and program coordinator of the National Newborn Screening Program for Sickle Cell Disease, many go undiagnosed and do not survive.

Barriers in the fight against SCD in Ghana

Aside from a lack of capacity to diagnose, access to SCD treatments — even when patients are diagnosed — poses a problem, explained Mary Ampomah, president, Global Alliance of Sickle Cell Disease Organizations. Yet, drugs are important in reducing symptoms and complications associated with SCD. They also help to improve the health of persons with SCD. Without treatment, a person living with SCD is forced to live with the pain that often accompanies SCD. This may mean lost days of work or school, affecting the person’s ability to learn and earn, as well as their mental health.
Mary Ampomah, president, Global Alliance of Sickle Cell Disease Organizations, explains how COVID-19 has exacerbated the challenges facing sickle cell disease patients.
“There is a huge financial burden when it comes to living with sickle cell disease because you need to take care of yourself as you get complications,” Ampomah said, adding that societal stigma for a person living with SCD is another dimension of the disease to contend with.

Sickle cell disease patients at Korle Bu Teaching Hospital in Ghana.
Sickle cell disease patients at Korle Bu Teaching Hospital in Ghana.
“People might see all those physical complications that [people with SCD] are having, and the stigma would increase in terms of labeling,” Ampomah said.
Numerous barriers prevent patients from receiving lifelong care for sickle cell disease.
Aside from access to medicines, experts listed numerous barriers preventing patients from receiving lifelong care: a lack of specialized SCD facilities and training for health care workers in SCD management, the costs of care, and poor compliance to treatments.
Side effects sometimes prevent patients from completing an entire course of treatment, Dei-Adomakoh explained. “Patients come, and they tell you that ‘I'm very tired, I don't think I can take the drugs anymore,’” she added.

Numerous barriers prevent patients from receiving lifelong care for sickle cell disease.
Numerous barriers prevent patients from receiving lifelong care for sickle cell disease.
A solution to the problem

In 2019, a public-private partnership — the Africa Sickle Cell Disease program — between the global medicines company Novartis, Ministry of Health of Ghana, Ghana Health Service, and the Sickle Cell Foundation of Ghana was launched to tackle these barriers. It aims to improve the lives of people with SCD in Ghana through the expansion of universal newborn screening and improved treatment via continuum care.

Professor Kwaku Ohene-Frempong, president at the Sickle Cell Foundation of Ghana and program coordinator of the National Newborn Screening Program for Sickle Cell Disease.
“We hope that this program we are building will eventually lead to universal newborn screening, and if government steps in and also supports their medications, then these children don't have to die young,” Ohene-Frempong said.

Professor Kwaku Ohene-Frempong, president at the Sickle Cell Foundation of Ghana and program coordinator of the National Newborn Screening Program for Sickle Cell Disease.
Professor Kwaku Ohene-Frempong, president at the Sickle Cell Foundation of Ghana and program coordinator of the National Newborn Screening Program for Sickle Cell Disease.

A nurse takes a blood sample from a sickle cell patient at Korle Bu teaching hospital.
A nurse takes a blood sample from a sickle cell patient at Korle Bu teaching hospital.
Under the agreement, centers of excellence dedicated to managing SCD are being set up in all regional capitals, complete with specialized SCD-trained medical teams. Further, Novartis has registered the drug hydroxyurea, the current standard of care, to treat SCD in Ghana, and 11 treatment centers and 3,400 patients have been given access to the medicine so far. In a study called REACH, hydroxyurea was shown not only to reduce pain but also to be safe for children with sickle cell anemia and “reduced the incidence of vaso-occlusive events, infections, malaria, transfusions, and death.”
Two years on, Nsiah-Asare said the program is making headway and that others should be committed to it and budget for such a program. Centers in 6 out of 10 regions have been set up so far.
Dr. Anthony Nsiah-Asare explains the objectives of the Africa Sickle Cell Disease program.
“It’s changed the quality of life of sickle cell positive patients or people living with SCD,” Nsiah-Asare said, adding that the centers that have been created are helping the country to diagnose SCD during newborn screenings.
“What we try to provide is a one-stop shop for SCD patients whereby you come, you have a lab to do your laboratory test for you, we have specialized clinics to take care of some of the complications that sickle cell patients are coming with,” Dei-Adomakoh said, explaining the need for a holistic approach that encompasses early screening and diagnosis, treatment, education, research, and advocacy.

Bringing innovation to patients

To facilitate effective disease management, the use of modern digital technology is also offering hope. In 2017, with support from Novartis, the Sickle Cell Foundation of Ghana worked with Dimagi, a social enterprise providing digital solutions, to develop and deploy a newborn screening app that serves as a registry making it easy to identify babies with SCD and refer them for further treatment.
“Right now, we have about 30,000 babies, all of whose data is collected on the app,” Ohene-Frempong — who is overseeing the Africa SCD program roll-out — said.
Professor Kwaku Ohene-Frempong explains how digital technology is helping health workers treat sickle cell disease patients.
In addition, the partners have developed a clinical management app that supports doctors in administering hydroxyurea and helps patients themselves manage their care. Having digital and real-time information at hand helps provide continuity of care, encourages patient follow-up, and supports disease management.



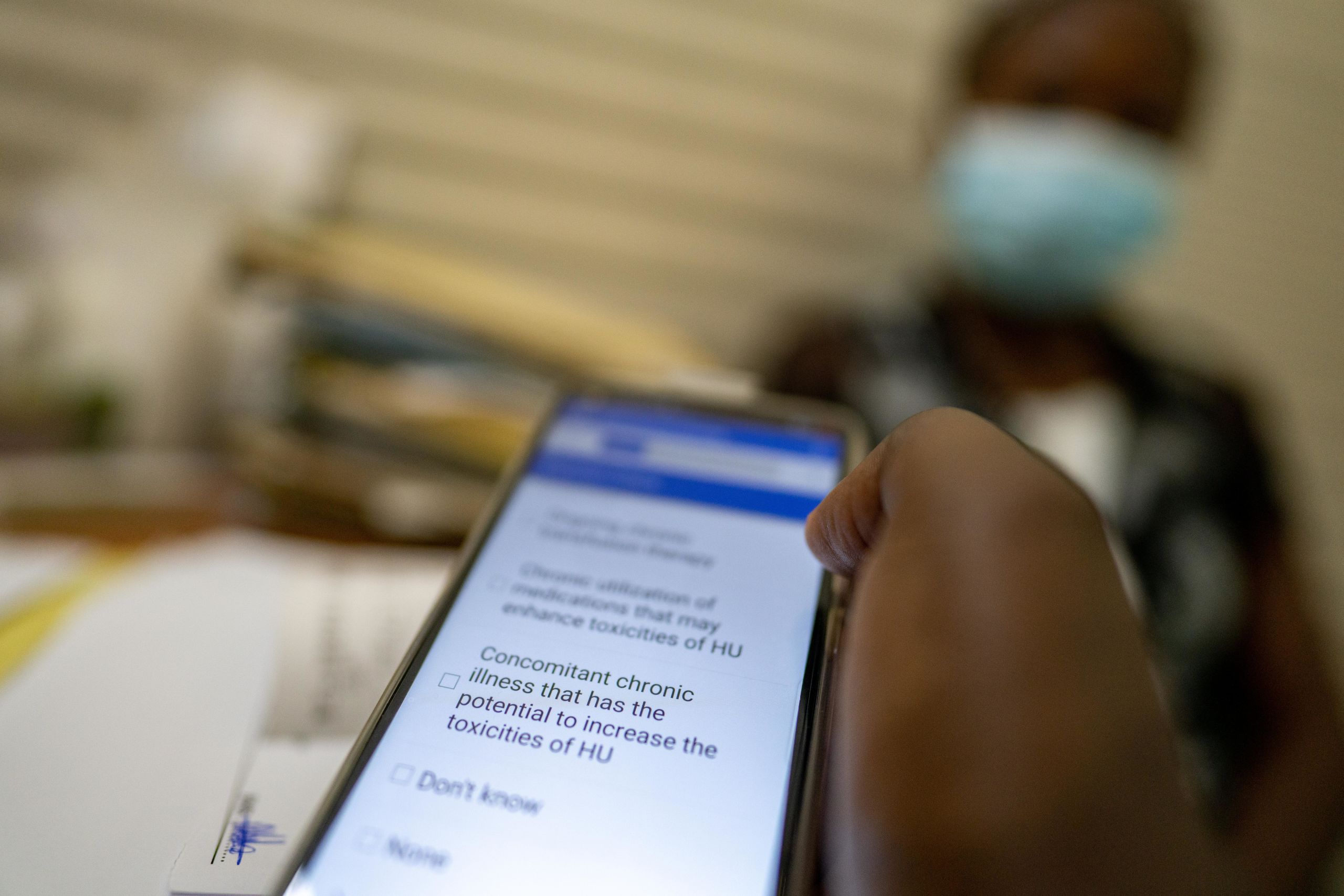
The clinical management app supports doctors in administering hydroxyurea and helps patients themselves manage their care.
The clinical management app supports doctors in administering hydroxyurea and helps patients themselves manage their care.
Beyond digital technology, Novartis has developed a child-friendly formulation of hydroxyurea that should be available toward year-end in Ghana, and is also conducting clinical trials on a next-generation biologic treatment — crizanlizumab, which is currently available in the United States and other countries around the world. Novartis aims to help build health care infrastructure and expertise in research for innovative treatments.
Crizanlizumab is an injectable medication given once monthly, Dei-Adomakoh — who is principal investigator for Novartis clinical trials — explained, adding that patients prefer having to only come in once a month for an infusion which lasts 30 minutes.
Dr. Yvonne Dei-Adomakoh explains how crizanlizumab, once approved, will help patients living with sickle cell disease manage their condition.
The immediate accessibility of the medicine once approved will be key to tackling SCD in the country, she said, adding that new drugs must also be made available and affordable in low- and middle-income countries.
While crizanlizumab awaits registration in Ghana, patients may also be eligible to participate in a Novartis Managed Access Program. MAPs provide patients with serious or life-threatening diseases who meet certain predefined criteria with access to therapies not yet approved or available in their country.
The future of the partnership

Although the partnership program still has much to achieve, gains are already being seen. The University of Ghana will be conducting monitoring and evaluation activities to assess the program’s impact.
According to Nsiah-Asare, data should be collected, analyzed, and used to encourage research around SCD and as a resource for the whole sub-Saharan Africa region.
With this in mind, Novartis plans to apply lessons from Ghana to expand the program to 10 other sub-Saharan African countries by 2022. Novartis is already on track to expand the activities to Tanzania, Kenya, and Uganda after signing three new memoranda of understanding in 2020.
As a next step, Novartis plans to work with other Ministries of Health “to further define the scope of each collaboration and explore opportunities for additional partnerships.”
“Once the goals of the Africa SCD program have been realized, and all SCD patients have access to screening, medicines, and care at no cost, SCD patients will have universal health coverage,” Nsiah-Asare said.


Text: John Yarney
Video/photos: Nana Kofi Acquah

