A new chapter in maternal nutrition:
Nepal’s journey toward MMS
What does it take to turn evidence into national health policy? Nepal is weighing a shift from providing iron and folic acid to multiple micronutrient supplements during pregnancy — a move aimed at improving the health of pregnant women and the next generation.
Sept. 3, 2025


Amid tightening global health budgets, governments are under increasing pressure to ensure that the investments they make are as high-impact as possible. Evidence-based policymaking has become a crucial part of this equation.
In Nepal, the government is paying close attention to maternal nutrition — a persistent challenge with wide-ranging consequences for families, communities, and the wider economy. Babies born to undernourished women are more likely to be premature or underweight, increasing the risk of complications in the earliest days of life. They can also face impaired physical and cognitive development, limiting their potential in adulthood.
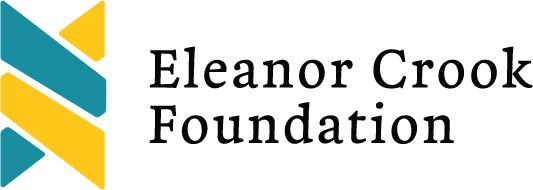
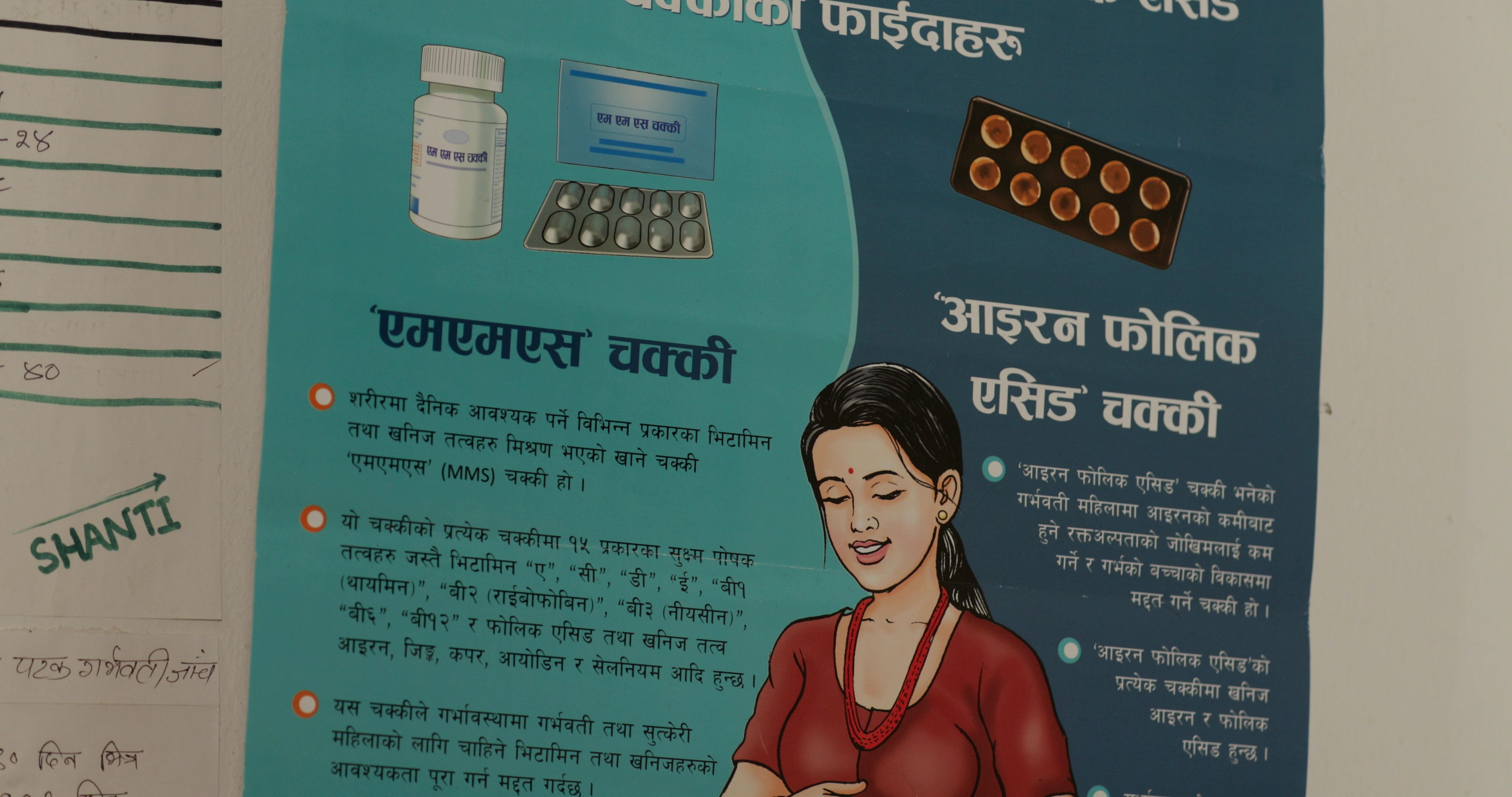
While the various causes of maternal malnutrition are complex to address, one potential intervention is gaining traction. Since 2003, women in Nepal have received iron and folic acid, or IFA — two important nutrients that help prevent anemia and support fetal development — throughout their pregnancies. Now the government is assessing whether a switch to a more comprehensive prenatal multivitamin — multiple micronutrient supplements, or MMS — could further improve health outcomes for mothers and babies alike. MMS contains 15 essential vitamins and minerals, including iron and folic acid, and has been proven to contribute to better pregnancy outcomes when compared to just taking IFA alone.
A study is currently underway into the acceptability and adherence to MMS among a sample of pregnant women in Lumbini province, southern Nepal. But translating these findings into national policy requires more than just evidence. It means mobilizing health workers, engaging pregnant women and their families, securing political backing at all levels of government, and overcoming logistical hurdles and financial constraints.









A mother's journey
When Sheela Rokaya gave birth to her first child four years ago, her circumstances were very different from what they are now. Living in India during the COVID-19 pandemic lockdown, she was isolated, fatigued, and undernourished. Her daughter, Deewansi, was born prematurely at just seven months and weighed just 1.5 kilograms. “She was too little,” Rokaya said, cupping her hands to show how small Deewansi was. “But when I took her in my hands, I was very happy.”
Sheela Rokaya, a young mother in Banke district, Lumbini province, recounts her challenging first pregnancy and what has changed since then.
Now living with her in-laws in Banke district, in Nepal’s Lumbini province, Rokaya has a better support system, access to nutritious foods, and regular visits to the local health center. As a participant in the MMS research study, Rokaya also received a daily dose of MMS from 13 weeks of pregnancy until the birth of her son, Divansh, who arrived healthy in January, weighing 2.6 kilograms.
Her experience is especially representative of women living in Nepal’s border areas, such as Banke district, where cross-border movement impacts maternal health. Rokaya’s story highlights the potential benefits of MMS and why Nepal is exploring a nationwide transition to these supplements.
“As far as I know, this medicine [supplement] will make my baby healthy and mentally strong. The baby will not be underweight.”
— Sheela Rokaya, a mother in Banke district


The MMS implementation research study, run by the government of Nepal in collaboration with NGO Helen Keller Intl and supported by Eleanor Crook Foundation, compares acceptability and adherence to MMS with that of IFA supplementation. A trial is underway in Lumbini province among a sample of pregnant women who are now taking the supplement daily throughout their pregnancies.
Pregnant women are invited to take part in the trial when they come for their first antenatal visit and, depending on the health facility, are given either MMS or IFA to take daily.





The barriers to good nutrition
At Chisapani health post, a small rural health center about 8 kilometers from Rokaya’s home, senior antenatal care provider Shanti Kumari Nepali is all too familiar with the signs of poor maternal nutrition. The situation has improved over the past two decades, in large part due to better nutritional counseling, but she still sees troubling cases. Of the roughly 20 pregnant women who visit the clinic each month, typically about three are underweight and have anemia, she said.
Senior antenatal care provider Shanti Kumari Nepali shares her experiences working in a small rural health centre in Banke district, and the nutrition challenges faced by the pregnant women who visit her there.
The causes range from poverty to limited awareness to certain cultural beliefs, said Kumari Nepali. In this border region, seasonal migration also has an impact. Frequent movement — especially when women return to their maternal homes across the border during pregnancy — can make it harder for health workers to maintain contact and ensure timely prenatal care. In addition, it can contribute to financial instability. “There are some families where the head of the family works in India throughout the year and comes home on festivals only. They pay their children's fees, parents' treatment, household expenses, and wife's treatment costs at that time,” she explained.
When women come to the health post for their antenatal visits — with eight recommended checkups throughout pregnancy — they receive nutritional counselling alongside routine services such as blood pressure checks, a hemoglobin test, and nutritional supplements. For those enrolled in the research study, Kumari Nepali also distributes either MMS or IFA, depending on their assigned group.
“When women follow my counseling, adopt healthy behaviors, and go on to have a safe delivery and a healthy baby, it gives me great satisfaction to know that both mother and child are doing well.”
— Shanti Kumari Nepali, senior antenatal care provider,
Chisapani health post in Banke district






Generating evidence for policy reform
Nepal has made significant progress in addressing the burden of maternal anemia, which in the late 1990s was estimated to afflict an estimated 75% of pregnant women and is now down to 34% nationally. Yet over the past 15 years, the prevalence of babies born with low birth weight has stagnated at approximately 12%, and malnutrition among children under 5 remains high.
A growing evidence base has shown that MMS has the potential to reduce low birth weight, anemia, and adverse pregnancy outcomes. In a major endorsement, MMS was added to the World Health Organization’s list of essential medicines in 2021.
Encouraged by these findings, Nepal’s Ministry of Health and Population, with support from nutrition NGO Helen Keller Intl, has been conducting research to assess the feasibility of a national transition. “We have to look at the cost factors. We have to look at the logistics, management challenges, and most importantly, we have to look at the acceptability by our clients, that is the pregnant women,” explained Bibek Lal, director of the family welfare division at Nepal’s Ministry of Health and Population.
“I think the global body of evidence that exists is the one which has given us confidence that MMS is the answer.”
— Bibek Lal, director of the family welfare division,
Nepal’s Ministry of Health and Population








Closing the gaps in prenatal care
Nepal’s cadre of female community health volunteers, or FCHVs, was formed in 1988 and is a cornerstone of maternal and child health in the country. As trusted community members, FCHVs go door to door to identify pregnant women and connect them with essential health services. Their role is especially critical in remote and hard-to-reach areas, including Nepal’s hilly and mountainous regions.
Female community health volunteer Rita Bhattarai, who lives and works in Dang district, Lumbini province, shares how she ensures pregnant women and mothers get the health and nutrition support they need.
Rita Bhattarai, an FCHV in Dang district in Lumbini province, looks after around 30 households. In addition to sharing vital nutrition information, volunteers like Bhattarai help build trust between the health system and local communities, often serving as the first point of contact for pregnant women. They also help to strengthen community bonds and support through regular “healthy mothers’ group” meetings — a space where women can connect, ask questions, and learn from one another.
As part of the MMS research trial, FCHVs like Bhattarai have been trained to counsel pregnant women on the benefits of the supplements and support consistent use.
“Challenges remain in reaching remote areas … deliveries and service provision are still very difficult there.”
— Rita Bhattarai, female community health volunteer, Dang district






Making it happen: What policy change takes
Leaders from across Nepal’s three levels of government — federal, provincial, and local — all have a role to play in making a potential nationwide scale-up of MMS a reality. A key challenge remains its higher up-front cost compared to IFA. However, the long-term benefits — measured in lives saved and disability-adjusted life years averted — make the investment worthwhile, Lal said.
Leaders from across Nepal’s three levels of government — federal, provincial, and local — discuss what's needed to scale up MMS across the country.
“The entire health system is ready to switch from IFA to MMS, but cost remains the main barrier,” he said. He emphasized the need for additional donor support to initiate a large-scale rollout. The Eleanor Crook Foundation, or ECF, is currently exploring cofinancing opportunities with the government to help overcome this barrier, and government-led discussions on a national MMS scale-up road map are already underway. Once MMS proves acceptable, effective, and in-demand among pregnant women across the country, the goal is to secure government funding at all levels to make it a permanent national program.
“Unless we ensure a safe pregnancy and delivery for every woman, our broader development goals are meaningless.”
— Prashant Bista, mayor, Nepalgunj sub-metropolitan city, Lumbini province





Ensuring quality, safety, and sustained supply
Ensuring a steady supply of MMS poses the biggest challenge for nationwide implementation, according to Narayan Dhakal, director-general of Nepal’s Department of Drug Administration. "Once you roll out a certain product, it has to be available around the clock," he said.
MMS is currently not manufactured in Nepal and is being imported from foreign suppliers for the purposes of the research trial. Developing local manufacturing capacity would reduce procurement costs in the long run and ensure a steady supply, but it also takes considerable time.
With ECF’s support, Nepal's Department of Drug Administration is working to include MMS and other nutrition products, such as ready-to-use therapeutic food, in the national essential medicines list, which would ensure it is treated as a priority in government procurement processes and provide sustainable funding beyond donor programs. This designation would also help to guarantee a stable market that could attract multiple manufacturers.
“Whatever comes, we'll be very much critically looking into the price side, the quality side, and the continuity of supply."
— Narayan Dhakal, director-general, Nepal Department of Drug Administration


What Nepal can teach others
Nepal's methodical approach — combining rigorous research while engaging communities, health workers, and government officials — could offer lessons for other countries struggling with maternal malnutrition. The transition from IFA to MMS represents more than a simple product switch — it's about making sure the health system better serves women and children. Through careful coordination, planning, and partnership, Nepal is building the foundation for healthier mothers and children.



Credits
Director, producer, and writer: Naomi Mihara
Photography and videography: Gorakh Bista
Public health expert & interpreter: Shijan Acharya
Video editing: Bhim Pariyar
Translators: Hiranya Joshi & Laxmi Maharjan
Editor: Rachael Perrett
With special thanks to the Helen Keller Intl Nepal team.
SPONSORED BY