Is Uganda Africa's role model when it comes to tackling hepatitis B?
As one of Africa's leading killers, what are the challenges to eliminating hepatitis B and what lessons can be learned from Uganda's gutsy approach?


KAMPALA, Uganda — At 9 a.m., the inside of the Mulago National Referral Hospital on the outskirts of Kampala, Uganda, sees patients sitting shoulder to shoulder in the waiting room. No chair is left vacant and no wall left un-leaned upon. Many of the patients arrived overnight, traveling great distances in the hope of guaranteeing a place in line and being seen by a doctor today.
Patients wait to be seen by a doctor at Mulago National Referral Hospital on the outskirts of Kampala, Uganda.
Patients wait to be seen by a doctor at Mulago National Referral Hospital on the outskirts of Kampala, Uganda.
Egalimaka is one of them. A businessman in Nakataka village, 120km (75 miles) north of Kampala, he’s suffering from chest pain — which he described as feeling like fire in his lungs — that may or may not be related to his hepatitis B diagnosis.
A viral infection that can go on to cause a chronic infection, cirrhosis, and liver cancer if not managed, hepatitis B is caused by the hepatitis B infection, or HBV, and can be fatal. Egalimaka is just one of the estimated 257 million people living with HBV worldwide. In Uganda, the prevalence stands at 4.3%, yet 52% endure a lifetime of exposure to the disease. This figure excludes children, yet HBV is predominantly contracted under the age of 5.
Unlike hepatitis C, there is no cure for hepatitis B, but the effects can be suppressed with nutritional balance and oral antiviral medicines — such as tenofovir — should the disease reach a chronic stage.
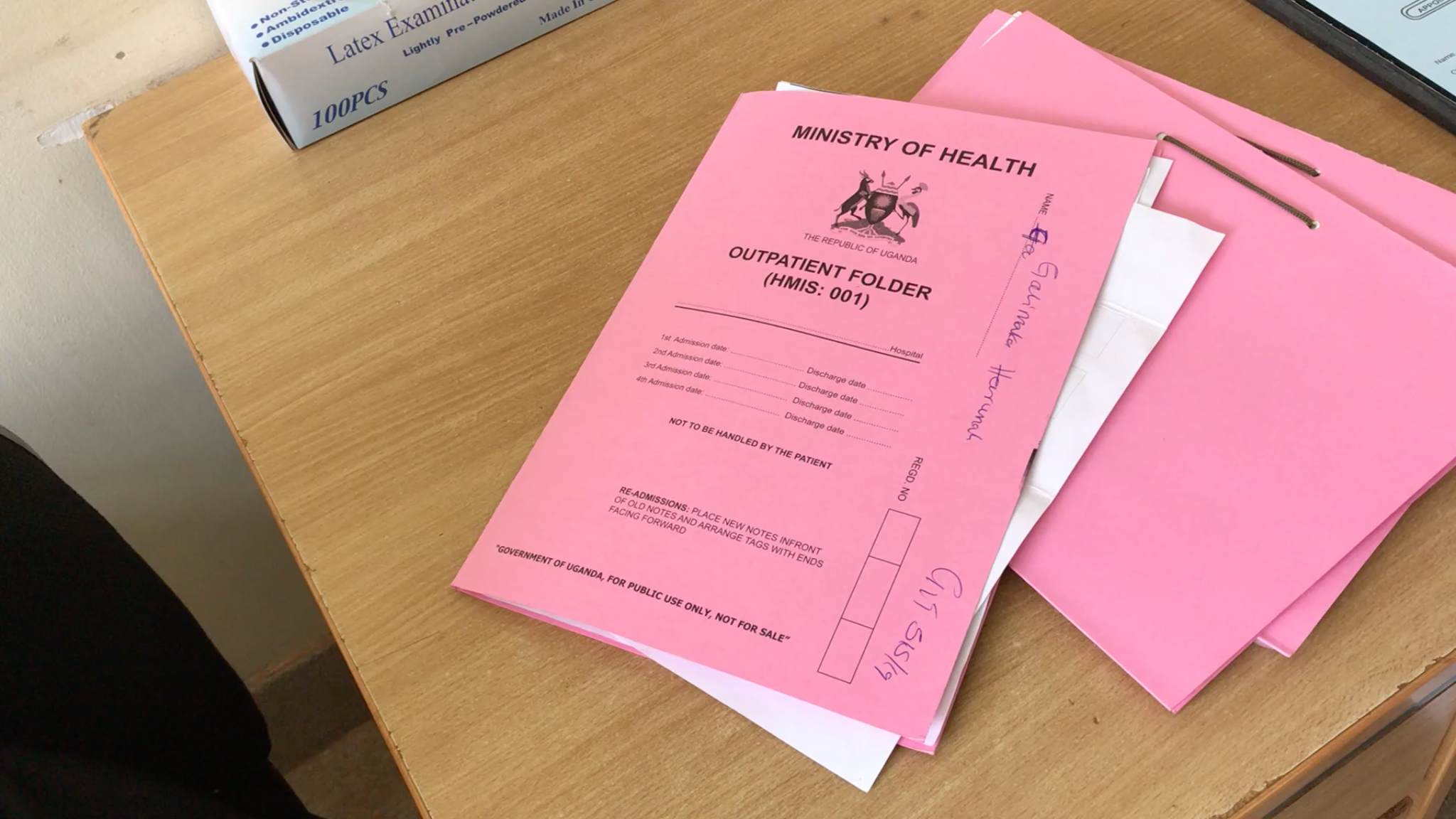
Egalimaka was diagnosed with hepatitis B in 2018, and while he was referred to Mulago National Referral Hospital some time ago, this is his first trip to the hospital that specializes in hepatitis diagnosis and treatment. After a consultation in a busy side room filled with nurses, the doctor will test his viral load levels — a measurement of how much HBV is in the blood — to determine whether he needs further treatment.


Egalimaka was diagnosed with hepatitis B in 2018
Egalimaka was diagnosed with hepatitis B in 2018
“They told me I should take greens, mangoes, I should not take cooking oil, I should not take alcohol … They counseled me that if I followed what the doctor said I should survive for some good years,” Egalimaka said, who lives with his wife and six children.


Mulago National Referral Hospital, a government-funded facility, offers liver function and viral load tests free of charge.
Mulago National Referral Hospital, a government-funded facility, offers liver function and viral load tests free of charge.
So far, Egalimaka says he has very few of the common symptoms — malaise, yellowing of the eyes, dark urine, sickness, and abdominal pain — and can’t be certain of how he contracted the disease. Like HIV/AIDS, the virus is transmitted via exposure to blood or other bodily fluids. Yet in Africa, dying of viral hepatitis is becoming a bigger threat than that of HIV/AIDS, malaria, or tuberculosis.
Dr. Opeto Moses, a medical officer and general practitioner in the gastroenterology clinic at the hospital, said that 80% of the patients he sees have hepatitis B. Most of them have been referred from different facilities, yet the diagnosis takes many by surprise, he said.
Despite the high prevalence at this hospital, in general, diagnosis rates remain low worldwide at 9%, making Egalimaka one of the lucky ones. The World Health Organization has set a target, as part of the first “Global Health Sector Strategy on Viral Hepatitis, 2016-2020,” for 30% of HBV-infected individuals to be diagnosed by 2020 and 90% by 2030.
Challenges in tackling hepatitis B
There are many challenges to achieving such targets. The main constraint is financial, said Kenneth Kabagambe, a hepatitis B patient and founding executive director of the National Organization for People Living with Hepatitis B — a patient-driven NGO advocating for the rights of hepatitis B patients in Uganda.
“This is a very expensive disease in terms of diagnostics,” Kabagambe said. “The majority of health facilities do not provide the test so it requires out-of-pocket expenses for the patient to actually access a diagnosis and also, in some cases, even the medicine.”
At Mulago National Referral Hospital — a government-funded facility that opened in 2016 to support its parent hospital — the liver function and viral load tests are undertaken free of charge, unlike in other facilities where there may be an associated cost.
The virus has been forgotten by big funding organizations, Kabagambe said. “This has discouraged some people in Africa [from] working on hepatitis because they have exhausted almost all of their earnings to tackle the issue,” he said, adding that it is unlikely there will ever be a global fund for hepatitis.
Access in remote settings to health care services is also an issue, Moses explained. Even if an individual can reach a local health facility, often it doesn’t have the equipment to correctly diagnose hepatitis B.
“Locally they cannot access the liver function test, they cannot access the renal function test,” he said, adding that oftentimes this means a referral to specialized facilities that could be further away and more costly to reach.
“Some of them end up not coming, some have financial challenges — they cannot board a bus and come this way — and some of them you will find, if they are not symptomatic, will not bother to come,” said Moses, adding that this increases the likelihood of the disease spreading.
Most governments are aware that hepatitis B isn’t adequately being diagnosed, said Dr. Kuku Appiah, director of medical and scientific affairs in Africa at Abbott, a global health care company.
“Previously, the challenge was that tests — other than Abbott’s — were not able to detect between an active and previous infection,” she said.

Steps to improve the diagnosis and detection of HBV
Despite these challenges, Uganda is already making great strides toward WHO targets and, according to the scorecard created by WHO to examine hepatitis prevalence, readiness, and response in the Africa region, the country is leading prevention efforts. Its hepatitis B “birth dose” — where an infant receives a vaccination in the first 24 hours of life — and childhood vaccinations exceed 90, while Uganda is one of only eight countries in the region providing subsidized testing and treatment for viral hepatitis.
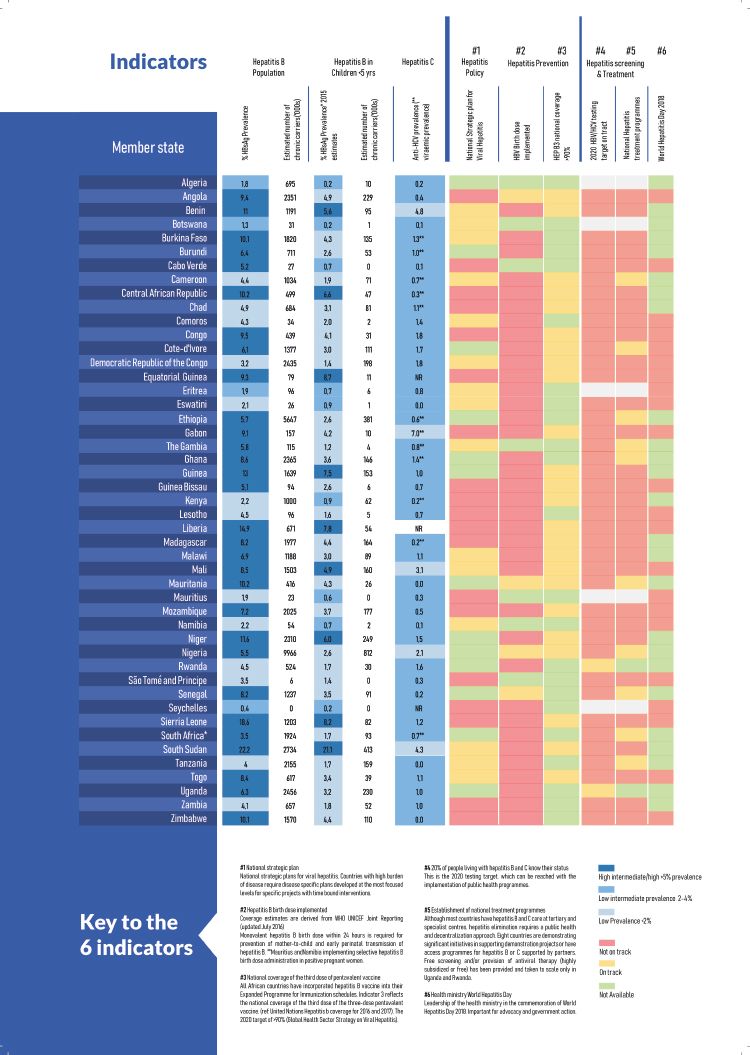
According to WHO's Hepatitis Scorecard Rwanda is leading hepatitis prevention efforts in the Africa region.
“I am extremely happy that WHO developed the scorecard to assess country performance in eliminating viral hepatitis in Africa — ever since we adopted the 2014 resolution on elimination of viral hepatitis — urging countries to put in effort, mobilize resources, and address the very big burden of viral hepatitis in Africa,” said Dr. Jane Aceng, Uganda’s minister of health.
In 2014, Uganda acknowledged viral hepatitis as a public health problem, established a hepatitis technical working group, created a national plan to tackle hepatitis B, and made a public decision to address the country’s endemic with an annual commitment of 10 billion shillings ($3 million).
Part of the plan was to increase its childhood immunization program to the screening and vaccination of those over the age of 15. Since 2015, the government has been conducting free screening in various parts of the country, vaccinating those who test negative, and providing free treatment to those who test positive. So far, more than 4 million people have been reached and 30% of Ugandans now know their hepatitis B status, making it the first country in Africa to exceed the 2020 target of 30%.

According to WHO's Hepatitis Scorecard Rwanda is leading hepatitis prevention efforts in the Africa region.
According to WHO's Hepatitis Scorecard Rwanda is leading hepatitis prevention efforts in the Africa region.


Dr. Opeto Moses says that 80% of the patients he sees have hepatitis B.
Dr. Opeto Moses says that 80% of the patients he sees have hepatitis B.
“The government of Uganda took a bold decision to vaccinate all the adults who have tested negative to protect them against hepatitis B, even if they may not need the vaccine,” Kabagambe said.
However, ensuring people receive all three doses of the vaccine is proving a challenge, according to Aceng. Coverage for the first dose can be as high as 91%, but that decreases to 68% for the second dose and 33% for the third, she explained.
“The majority of the people we talk to mention forgetting as one of the highest causes [of missing a vaccine appointment], because there is a six-month gap in between and the majority of the people forget,” Aceng said, adding that another challenge is a lack of transport to a health facility. “I want to appeal to the population, please come back and get your third dose so you are certain you are 100% protected from viral hepatitis B.”
Kabagambe argued that Uganda needs to invest more in community mobilization and awareness raising so that people will actively seek a diagnosis and return for their vaccination doses. Stigma and misinformation about hepatitis can lead to a lack of willingness to be tested. “The government really needs to revisit its strategies and fund more of the awareness activities and community mobilization in order to create demand for scaling up the testing.”
Public information campaigns for other diseases such as measles and polio have cost the country over $30 million, Aceng said. “It’s not easy to run a campaign when we have very limited partners supporting us in this initiative.”
Abbott’s new point-of-care rapid test aims to enable faster identification of those with the virus.
Abbott’s new point-of-care rapid test aims to enable faster identification of those with the virus.
While that may be the case, one partner the country is working with to improve diagnosis of hepatitis B is Abbott. Together they piloted Abbott’s new point-of-care rapid test — the Determine HBsAg 2 — which aims to enable faster identification of those with the virus. The thin strip of plastic encases a tiny test that collects a blood sample from a finger and reveals a result in 15 minutes.
“We’re able to provide an affordable and accessible solution once [governments] have decided to undertake screening programs for their populations,” Appiah said, highlighting new technologies as critical to the fight against hepatitis B. “It’s the only way that you can get high-level, laboratory comparable tests to people in the most remote sites.”


The new test reveals a result in 15 minutes.
The new test reveals a result in 15 minutes.
The trial showed the test’s high sensitivity, ability to diagnose, and ease of use. The next step is for Uganda and other countries to register and procure the test so that health care workers in more remote settings can instantly diagnose a patient, therefore speeding up treatment plans and reducing transmission rates.
It’s critical this screening process runs as part of bigger campaigns to screen, identify and treat people, Appiah said. “We’re encouraging countries to put that holistic program in place.”
She called upon other organizations also working to bring down the cost of hepatitis B testing and treatment, to ensure any innovations are accessible in individual countries down to the local level.
For someone like Egalimaka, that would mean a doctor’s visit without hours of travel time, an overnight stay, and a potential loss of a day’s earnings.
“My plans for the future are to take care of my children so they can go to school and to care for my family,” he said.